"When a lateral impact collides with a planted foot, the inner knee is subjected to a violent opening force. Restoring stability depends not on structural splinting, but on training the surrounding muscle chain to act as an active shield."
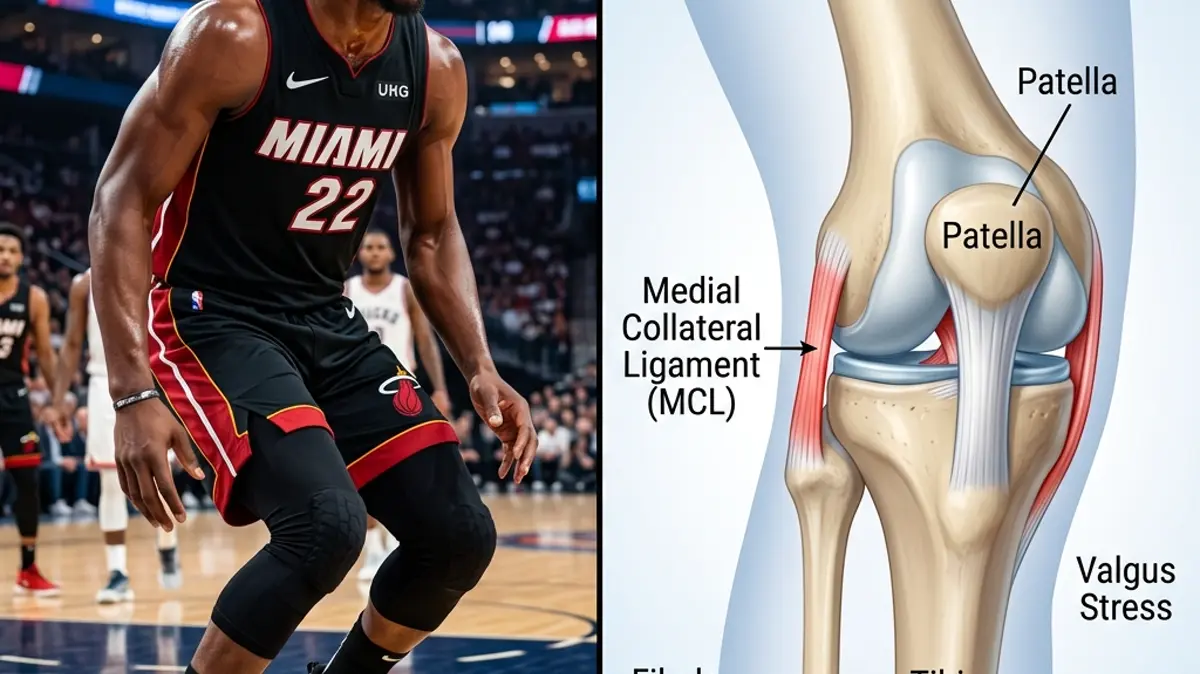
Jimmy Butler's aggressive playing style and physical drive to the basket make him a cornerstone of his team. However, absorbing heavy impacts during jump landing and lateral cutting puts immense pressure on his knee ligaments. When a player of his caliber sustains an MCL sprain, it highlights the vulnerability of the medial knee joint during high-energy basketball maneuvers.
Many athletic coaches rush players back with heavy bracing and painkillers. In reality, a compromised MCL leaves the knee vulnerable to chronic rotational instability and secondary meniscus damage. Reconditioning the joint requires a structured recovery program that focuses on dynamic knee alignment.
Restoring elite lateral stability demands a deep look at knee valgus forces. By evaluating muscle activation patterns and utilizing targeted jimmy butler injury rehabilitation protocols, we can rebuild joint integrity. This article explores the pathology of medial ligament trauma, conservative recovery phases, and lateral chain stabilization.
The Biomechanics of Valgus Collisions and Medial Ligament Injury
The medial collateral ligament (MCL) is the primary static stabilizer against valgus stress (inward buckling of the knee) and external rotation of the tibia. In basketball, valgus loading commonly occurs in two ways: either a direct contact blow to the outer side of the thigh while the foot is fixed, or a rapid, uncoordinated change of direction that forces the knee to collapse inward.
When the knee collapses into a valgus position under body weight, the distance between the medial femoral condyle and the tibia increases rapidly. This mechanical separation stretches the fibers of the MCL. If the forces exceed the ligament's elastic threshold, the fibers experience micro-tearing or a complete structural rupture.
Unlike the ACL, the MCL is an extra-articular ligament with a rich vascular supply. This blood flow facilitates a robust inflammatory and tissue-repair response, enabling non-surgical healing. However, if the knee is not protected from lateral forces in the early stages, the ligament heals in a lengthened, lax state, causing chronic joint instability.
Clinical indicators for medial collateral ligament healing and stability:
- 1Valgus Load ResistanceThe MCL provides up to 80% of the knee's passive resistance to valgus force at 25 degrees of flexion.
- 2Blood Supply AdvantageDue to high vascularity, Grade 2 tears show complete structural union within 6 weeks of controlled loading.
- 3Dynamic Control DeficitWeakness in the gluteus medius increases dynamic knee valgus collapse by 25% during single-leg landings.
- 4Surgical Avoidance RateOver 95% of isolated Grade 1-3 MCL sprains are successfully managed without surgical intervention.
The Clinical Opinion: Progressive Bracing vs. Rigid Plaster Casting
"Treating an MCL sprain requires early protection from valgus loads, but the joint must never be locked in a rigid plaster cast. In my clinical opinion, complete joint immobilization leads to rapid quadriceps inhibition and patellar stiffness. By using a hinged knee brace that limits lateral movement while allowing free flexion and extension, we protect the healing ligament while keeping the thigh muscles active."
Traditional recovery protocols often involved locking the knee in a straight splint for several weeks. While this keeps the ligament safe, it causes severe muscle wasting and long-term stiffness. Modern physical therapy utilizes a hinged brace to allow safe sagittal movement while blocking harmful lateral shear forces.
Controlled movement within a safe range stimulates mechanoreceptors in the joint, improving balance and reducing pain. As tissue healing progresses, we gradually remove the brace and introduce exercises that challenge the dynamic stabilizers of the knee, such as the gluteus medius and vastus medialis obliquus (VMO).
Multi-Stage Medial Ligament and Lateral Stability Protocol
Restoring a basketball player's knee to peak performance requires a systematic progression that balances ligament protection with functional strength.
Phase 1: Inflammatory Control and Sagittal Range (Weeks 1-2)
The primary focus is on protecting the medial joint line and restoring full knee extension. The athlete wears a hinged knee brace locked to allow 0-90 degrees of flexion, avoiding any lateral or pivoting movements. Ice, compression, and elevation are used to manage swelling.
We initiate quadriceps activation exercises to prevent muscle inhibition. The athlete performs straight leg raises and quad sets, focusing on tightening the inner thigh muscles. These exercises are performed in 3 sets of 15 repetitions twice daily.
Passive range of motion is performed within the brace limits. The athlete sits on a table and slowly bends and extends the knee, avoiding any pain or pressure on the inner joint line.
Phase 2: Closed-Chain Strength and Gluteal Integration (Weeks 3-4)
Once the athlete can walk without a limp, we unlock the brace and progress to weight-bearing exercises. The athlete performs bilateral squats to 60 degrees, using a resistance band around the knees to prevent them from caving inward. This activates the hip abductors to shield the MCL.
We introduce single-leg balance exercises on stable surfaces. The athlete stands on the injured leg while keeping the hips level and the knee aligned over the second toe. This trains the ankle and hip to stabilize the knee joint dynamically.
Hip abduction exercises are performed in side-lying and standing positions. Strengthening the gluteus medius is crucial, as it controls the lateral alignment of the femur and prevents dynamic valgus collapse during play.
Phase 3: Plyometric Loading and Court-Specific Pivoting (Weeks 5-8)
The final phase focuses on high-velocity shock absorption and lateral movement capacity. The athlete begins light double-leg vertical jumps, focusing on soft landings with optimal knee alignment. This is progressed to single-leg hopping drills as tolerated.
Lateral shuffling and diagonal cutting drills are introduced on the court. The athlete performs controlled, low-speed cuts, gradually increasing velocity and angle. The knee is monitored closely for any pain or instability during sudden stops.
Sport-specific conditioning, including jumping and shooting drills, is integrated. The athlete returns to full team practice only after passing a battery of functional tests, including a 90% score on the single-leg hop test compared to the uninjured leg.
Correcting the Hip-Knee Biomechanical Axis
An MCL injury is often a symptom of poor biomechanical control at the hip and ankle. If the hip abductors are weak, the femur rotates inward and collapses, forcing the knee into a valgus position. Similarly, stiffness in the ankle joint restricts normal dorsiflexion, causing the foot to pronate and pull the knee inward.
To prevent future ligament sprains, the rehabilitation program must target these surrounding joints. Rebuilding ankle mobility and hip strength ensures that the knee remains centered during explosive movements. A balanced kinetic chain is the key to athletic longevity.
For more lower extremity rehabilitation guides, read our analyses of ACL tear recovery protocols, meniscus tear conservative rehab, and runner's knee hip reconditioning. You can also view our athletic injury updates on Rickea Jackson's WNBA ACL reconstruction, Luka Doncic's ankle sprain recovery, and Joel Embiid's knee meniscus tear biomechanics.
Featured image attribution: Left panel displays a visual representation of basketball player Jimmy Butler showing knee discomfort on court. Right panel shows a detailed 3D medical anatomical illustration highlighting the knee joint structure, medial collateral ligament (MCL), patellar tendon, and valgus stress forces. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
