"A tendon is a dynamic spring, not a static cable. When chronic loading spikes exceed the tissue's metabolic repair rate, the cellular matrix degenerates, transferring high-energy landing impacts directly into the bone."
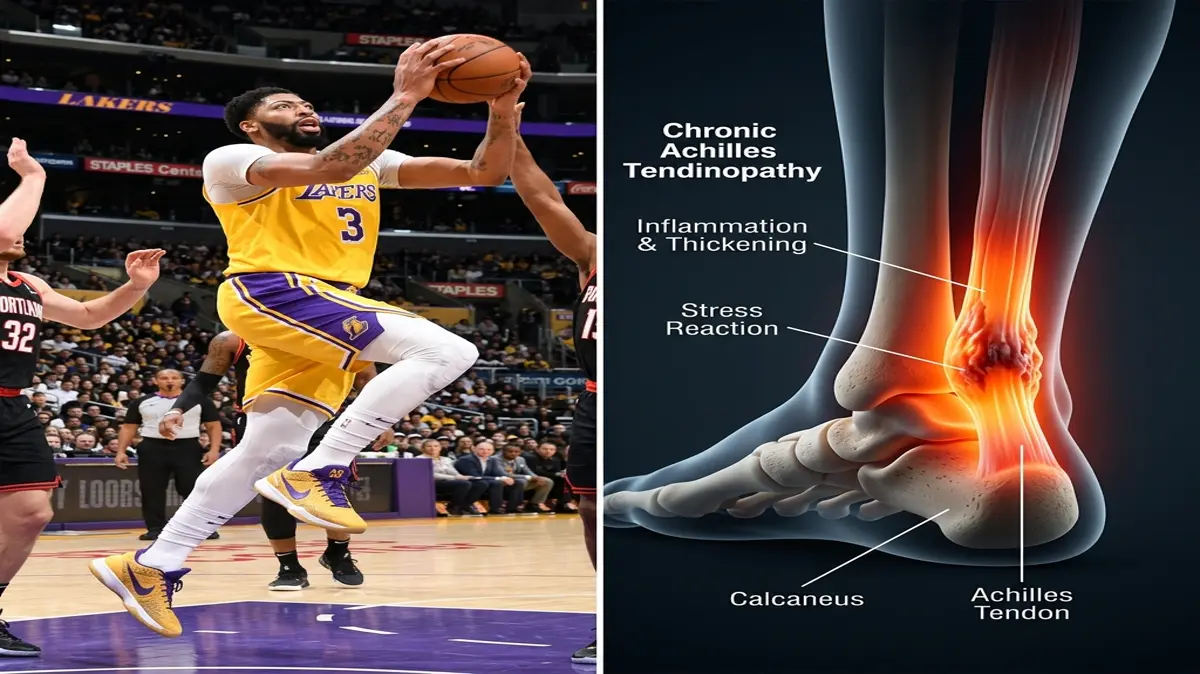
Anthony Davis's elite career in professional basketball has been marked by dominant performances and recurring lower extremity injuries. Among these, chronic Achilles tendinopathy and secondary bone stress reactions in the foot represent significant biomechanical challenges. Managing these issues in a seven-foot athlete requires a deep understanding of load distribution and tendon physiology.
Standard sports medicine often prescribes rest and pain management to address tendon irritation. However, passive recovery does not restore the tendon's load-bearing capacity. Rebuilding a durable tendon requires a system of progressive mechanical loading paired with joint mobilization to correct kinetic chain compensations.
Restoring peak court performance requires addressing the specific forces acting on the foot. By analyzing his landing mechanics and using targeted anthony davis injury rehabilitation, we can restore joint and tendon durability.
This article reviews the biomechanics of Achilles degradation, bone stress physiology, and progressive reconditioning stages.
The Biomechanics of Achilles Tendinopathy and Bone Stress
In basketball, jumping and landing subject the Achilles tendon to forces up to eight times the athlete's body weight. This extreme load is stored and released elastically to power explosive movements. If the calf-tendon complex lacks sufficient stiffness, this energy cannot be absorbed, leading to micro-tearing in the tendon's collagen matrix.
Over time, repetitive overload without adequate recovery triggers a degenerative process known as tendinosis. The tendon's organized Type I collagen fibers break down, replaced by weaker Type III fibers and fluid accumulation. This structural degeneration weakens the tendon, transferring high landing impacts directly into the surrounding foot bones.
When the heel and midfoot bones absorb these forces repeatedly, the bone tissue begins to break down faster than it can rebuild. This imbalance leads to a bone stress reaction, which presents as deep ache and localized swelling. If ignored, the stress reaction can progress to a full stress fracture, requiring months of immobilization.
Achilles tendinopathy affects up to 15% of all competitive basketball players. Additionally, foot stress reactions account for nearly 20% of all lower extremity bone injuries in elite sports. Rebuilding joint health requires structural tendon remodeling paired with rigid impact management.
Key clinical parameters tracking tendon remodeling and bone stress healing:
- 1Tendon DegenerationType III collagen accumulation reduces the tendon's tensile load-bearing capacity by 40%.
- 2DF RestrictionA loss of 10 degrees of ankle dorsiflexion increases Achilles landing tension by 30%.
- 3Bone Healing WindowResolution of a bone stress reaction requires 4 to 6 weeks of non-impact conditioning.
- 4Load ProgressionHeavy slow resistance training stimulates tenocyte alignment and increases collagen density within 8 weeks.
The Clinical Opinion: Heavy Slow Resistance vs. Passive Treatment
"Treating chronic tendinopathy in a tall, high-impact basketball player demands heavy slow resistance (HSR) training. In my clinical opinion, passive treatments like ultrasound or absolute rest fail to stimulate tendon tissue remodeling. By applying high-load, slow contractions, we trigger tenocyte activity to lay down strong, aligned collagen, restoring the tendon's spring-like qualities."
Passive treatments fail to address the underlying structural weakness of the degenerated tendon. Rest may reduce acute pain, but the tendon remains weak and disorganized once the athlete returns to the court. Heavy slow resistance training is the gold standard for restoring tendon integrity.
HSR involves slow, high-load calf raises that load the tendon in both the concentric and eccentric phases. This slow mechanical strain stimulates the tendon cells (tenocytes) to synthesize new collagen and realign the matrix. As tendon stiffness increases, shock absorption improves, protecting the underlying bone from excessive landing forces.
Multi-Stage Achilles and Bone Stress Rehabilitation Protocol
Reconditioning an athlete's ankle requires a progressive program that allows bone healing while building tendon load-bearing capacity.
Phase 1: Unloading and Isometric Loading (Weeks 1-3)
The initial phase focuses on allowing the bone stress reaction to settle while preserving muscle activation. The athlete wears a protective walking boot or limits impact to prevent bone loading. Cardiovascular fitness is maintained via pool training and cycling.
Mid-range isometric calf holds are performed to maintain muscle tone and reduce tendon pain. The athlete sits and presses their toes against a solid block, holding the contraction for 45 seconds. This exercise is performed in 5 repetitions with 2-minute rests between holds.
Manual ankle mobilizations address talocrural joint stiffness. The physical therapist performs posterior talar glides to improve dorsiflexion range of motion. Restoring joint mobility reduces compensatory forces on the Achilles during walking.
Phase 2: Heavy Slow Resistance and Calf Reconditioning (Weeks 4-6)
Once bone tenderness has resolved, we transition the athlete out of the boot and introduce progressive loading. The athlete begins heavy slow resistance training using a calf raise machine. The movement is performed slowly, taking 3 seconds to rise and 3 seconds to lower.
Exercises are performed in 3 sets of 8 repetitions at 70% of maximum capacity, twice weekly. We monitor the tendon closely for any pain that persists for more than 24 hours after exercise. Adjustments to the load are made based on tissue response.
Intrinsic foot muscle strengthening, such as towel scrunches and arch lifts, is added. Strengthening these small support muscles improves the foot's natural shock-absorption capacity. This stabilization reduces the mechanical stress placed on the tarsal bones.
Phase 3: Plyometric Loading and Return-to-Sport (Weeks 7-10)
The final phase focuses on rebuilding explosive tendon power and court-specific skills. The athlete begins light plyometric training, starting with double-leg hopping before progressing to single-leg bounds. These exercises train the tendon to store and release elastic energy.
Court-specific running drills are introduced, focusing on acceleration, deceleration, and lateral cutting. The athlete performs these movements at progressive intensities twice weekly. Proprioceptive training on unstable surfaces restores ankle balance.
The athlete is gradually integrated back into team practices and competitive games. We continue to monitor ankle range of motion and local tendon thickness throughout the season. Continued HSR maintenance drills are performed weekly to preserve tendon health.
Addressing Kinetic Chain Compensations
An Achilles tendon injury is often part of a wider pattern of lower limb kinetic chain dysfunction. Restricted ankle mobility limits hip extension, forcing the gluteus maximus to underperform during sprinting. This gluteal weakness leads to hamstring overload and pelvic instability.
To address these compensations, the program includes gluteal strengthening and hip flexor stretching. Ensuring optimal hip mechanics reduces the workload on the calf-tendon complex. Restoring balance to the entire lower limb is essential for achieving long-term joint safety.
For more lower extremity rehabilitation guidelines, read our detailed guides on Achilles tendinitis HSR protocols, restoring ankle stability after sprains, and plantar fasciitis posterior chain release. To understand sports-specific ankle and leg mechanics, view our analyses of Kevin Durant's Achilles rupture, Harry Kane's ankle sprain recovery, and Novak Djokovic's meniscus tear surgery recovery. You can also review Christian McCaffrey's Achilles tendinitis recovery.
Featured image attribution: Left panel displays basketball player Anthony Davis jumping for a rebound on the court. Right panel shows a clinical 3D medical illustration highlighting the ankle joint, Achilles tendon thickening, and local bone stress reaction points. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
