"Retraining a ruptured or chronically degenerated Achilles tendon is like tuning the high-tension steel rigging rigging of a racing yacht—if you simply leave the boat docked in port, the structure never adapts, and if you tighten it too fast under high winds, it snaps."
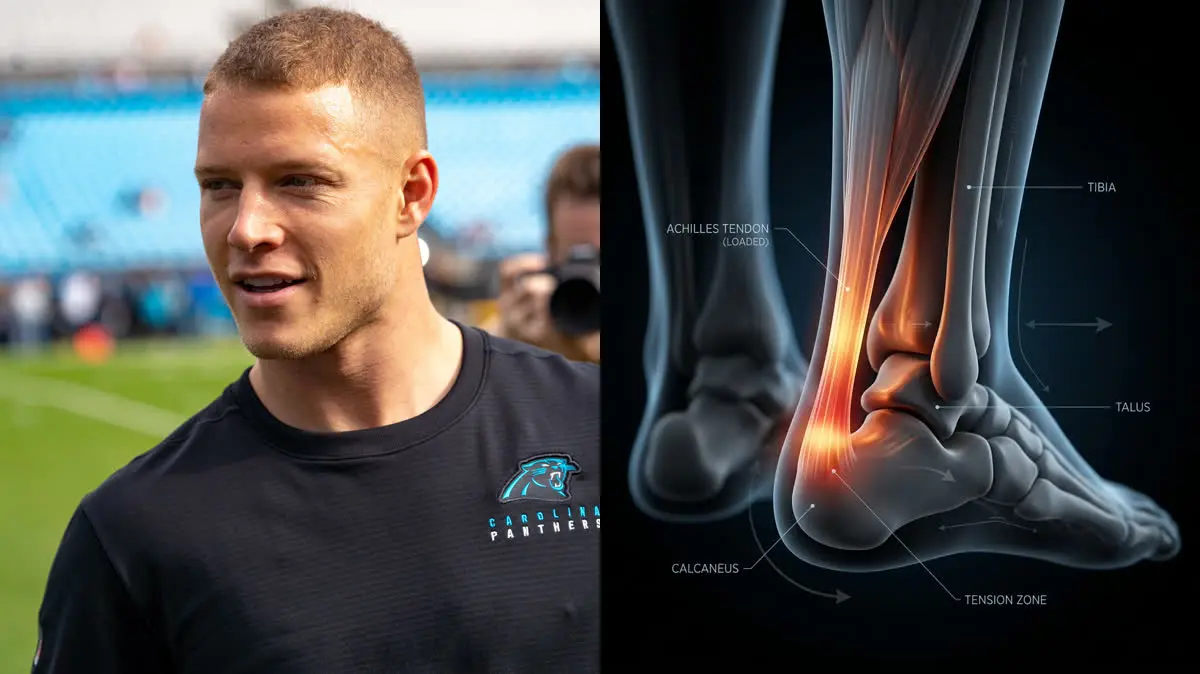
When San Francisco 49ers superstar running back Christian McCaffrey was sidelined during his historic 2024–2025 campaign, NFL fans were left in shock. The official diagnosis—bilateral Achilles tendinitis that eventually required him to travel to Germany for specialized treatment—sent search engines into overdrive.
For any explosive athlete, hearing that the tendon at the back of their heel is inflamed triggers immediate anxiety. The knee-jerk reaction is almost always to rest completely, wear protective walking boots, and perform aggressive static stretching to lengthen the calf.
However, elite sports medicine has shifted away from this passive model. Tendons are highly specialized, dense structures that do not possess a rich, flowing blood supply. When you rest them completely, they lose their mechanical stiffness, making them even more vulnerable to re-injury upon return.
To resolve chronic degeneration and return to explosive movement, athletes must implement progressive high load tendon exercises. In this clinical analysis, we will deconstruct the biomechanical forces of christian mccaffrey achilles tendinitis, evaluate the role of calf muscle biomechanics running, and outline the exact protocols used in modern achilles tendinitis rehabilitation nfl programs.
The Biomechanical Demands of a Running Back
A running back's career is defined by acceleration, deceleration, and high-velocity cutting. With every explosive push-off or sudden stop, the calf-Achilles complex acts as a primary energy accumulator, absorbing and returning massive kinetic energy.
The Achilles tendon behaves like a dynamic spring. During the stance phase of running, it stretches to store energy and recoils during toe-off, amplifying the force generated by the gastrocnemius and soleus muscles.
If this spring loses its structural integrity due to micro-tearing and disorganized collagen fibers, it can no longer transmit force efficiently. The muscle must work harder, causing rapid fatigue and placing excessive shear stress on the insertion point, leading to chronic sports physical therapy heel pain.
Biomechanical tracking shows that running and cutting place a mechanical load equal to 6 to 8 times an athlete's body weight directly on the Achilles tendon. For a 210-pound running back, that means managing up to 1,680 pounds of force with every single stride.
Furthermore, clinical trials show that Heavy Slow Resistance (HSR) protocols achieve success rates of over 70% in chronic tendinitis cases, compared to less than 35% for passive rest and stretching.
In terms of safety metrics, athletes returning to play with a Limb Symmetry Index (LSI) of less than 90% in calf strength are 3 times more likely to suffer a tendon re-tear or rupture, proving the need for objective testing.
Why Complete Rest and Passive Stretching Fail the Tendon
When your heel bone feels stiff and sore, pulling your toes back in a deep calf stretch seems logical. You believe you are lengthening the tight tendon.
My strong clinical opinion is that passive stretching is highly detrimental to an insertional Achilles tendinopathy. When you pull the foot into deep dorsiflexion, you press the inflamed tendon directly against the hard, bony corner of the heel bone (calcaneus).
This compression creates localized shearing forces that actively aggravate the micro-tearing, locking the tendon into a chronic cycle of degeneration. To heal, the tendon must be loaded, not stretched. Retraining must utilize high-load isometrics and slow, heavy eccentrics to stimulate tenocyte activity and realign the chaotic collagen matrix.
If you are also experiencing pain under the arch of your foot, understanding how releasing the posterior chain heals plantar fasciitis can ensure your entire lower leg biomechanics are balanced.
The 3-Phase High-Load Achilles Protocol
To stimulate new, healthy collagen formation and resolve chronic heel discomfort, perform this progressive routine 3 times per week:
-
1Isometric Heel Raise Holds (Pain Modulation Phase) Stand on a flat floor. Rise onto your tiptoes on both feet, then shift 70% of your weight to the injured leg. Hold this position for 45 seconds without moving. Repeat 5 times, resting 60 seconds between holds. The sustained tension triggers a biological analgesic effect, reducing tendon pain for up to several hours.
-
2The 6-Second Heavy Calf Raise (Remodeling Phase) Stand on the edge of a step with your heels hovering. Take a full 3 seconds to raise up onto your tiptoes, and a full 3 seconds to lower back down. Perform 3 sets of 10 repetitions with a weighted backpack or holding dumbbells. The slow speed removes elastic recoil, forcing the tendon to bear the mechanical load.
-
3Plyometric Reconditioning (Elastic Spring Phase) Once heavy loading is pain-free, gradually reintroduce elastic forces. Begin with double-leg pogo hops (jumping from the ankles with minimal knee bend) for 3 sets of 30 seconds. Progress to single-leg hops to rebuild the tendon's capacity to absorb and release energy rapidly.
Just like in Kevin Durant's Achilles rupture recovery, progressive loading is the only way to restore the tendon's maximum load tolerance.
Take Control of Your Recovery
Achilles tendinitis is not a permanent sentence of weakness; it is a structural capacity issue. By replacing passive rest and stretching with progressive, heavy slow loading, you can systematically rebuild the tendon matrix and return to your sport with confidence.
To understand how to get started on a complete self-treatment plan, read our comprehensive guide on Achilles Heavy Slow Resistance protocols.
Are you ready to stop resting and start actively strengthening your foundation? Perform your first set of isometric holds today and take control of your athletic future.
Featured image attribution: "Christian McCaffrey 2019.jpg" by Merson (original photograph by All-Pro Reels), licensed under CC BY-SA 2.0. Modified by cropping and compositing with an AI-generated clinical visualization.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
