"The shoulder blade is the anchor of the arm. If the anchor moves erratically during a 120-mph serve, the rotator cuff is pinched against bone, turning a high-performance movement into chronic impingement."
Coco Gauff's explosive game and high-velocity serves have established her as one of tennis's elite athletes. However, serving at speeds exceeding 120 mph subjects the shoulder joint to extreme mechanical strain. Her struggles with rotator cuff tendinopathy and secondary scapular dyskinesis highlight the complex biomechanics of overhead athletes.
Standard athletic recovery often relies on passive stretching and anti-inflammatory medication. While these methods temporarily reduce discomfort, they do not address the underlying muscular imbalances or restore tendon tissue structure. Rebuilding a durable shoulder requires a progressive strengthening program that restores scapular control and enhances kinetic chain integration.
Restoring elite serving mechanics requires analyzing the exact phases of the overhead motion. By studying shoulder muscle dynamics and using targeted coco gauff injury rehabilitation, we can rebuild a highly stable joint.
This article reviews the biomechanics of serve-induced trauma, scapular movement pathology, and progressive shoulder conditioning stages.
The Biomechanics of the Tennis Serve and Rotator Cuff Overload
The tennis serve is a complex whole-body movement that relies on a kinetic chain starting from the legs, traveling through the core, and releasing through the arm. During the acceleration phase, the arm is whipped forward, generating massive rotational force. Immediately after ball contact, the rotator cuff muscles must contract eccentrically to decelerate the rapidly moving arm.
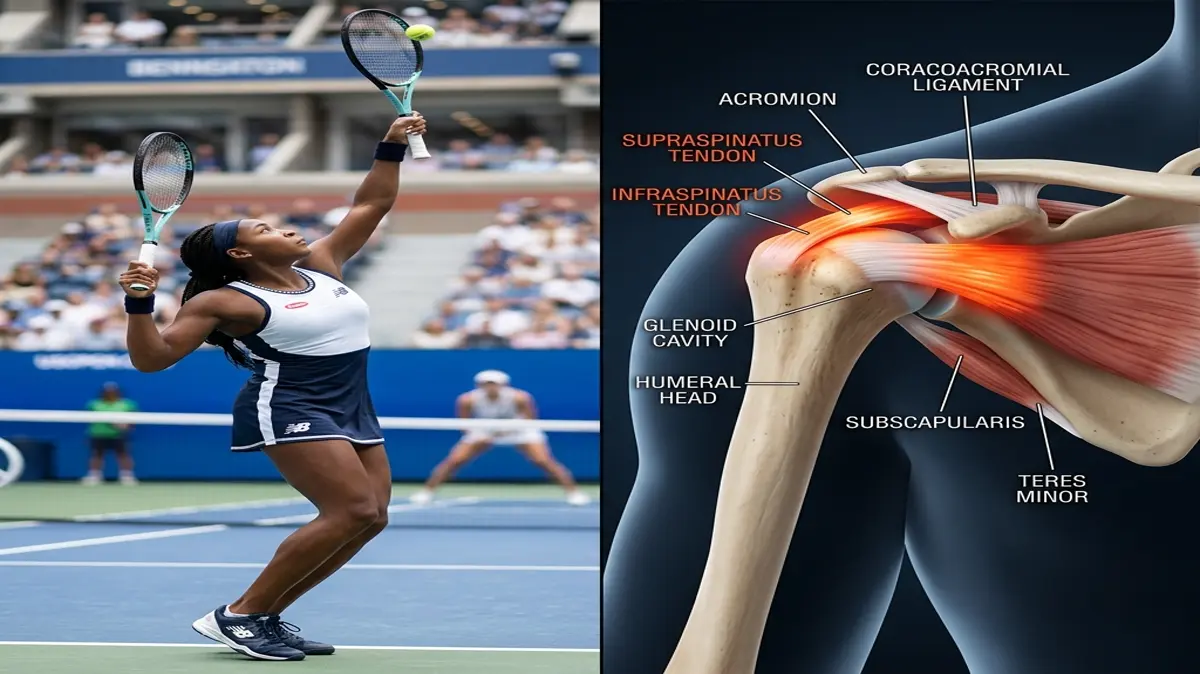
This deceleration phase places extreme eccentric tension on the supraspinatus, infraspinatus, and teres minor tendons. If these muscles lack sufficient strength or fatigue during a match, the mechanical stress exceeds the tendon's structural limit. This repetitive overload causes micro-tearing and chronic tendon thickening, leading to painful tendinopathy.
Furthermore, if the shoulder blade (scapula) fails to rotate upward smoothly to make room for the arm, the subacromial space is reduced. This movement fault, known as scapular dyskinesis, causes the acromion bone to pinch the rotator cuff tendons during overhead movements. This mechanical impingement accelerates tissue degradation, causing pain and weakness.
Rotator cuff injuries account for nearly 20% of all tennis-related shoulder traumas. Additionally, up to 70% of overhead athletes with chronic shoulder pain display some degree of scapular dyskinesis. Reconditioning the joint requires restoring the strength and coordination of both the rotator cuff and scapular stabilizing muscles.
Key clinical parameters tracking rotator cuff recovery and scapular control:
- 1Subacromial SpaceScapular dyskinesis can reduce the subacromial space by up to 30%, increasing impingement risk.
- 2Deceleration LoadEccentric deceleration forces on the rotator cuff can reach up to 1.5 times the athlete's body weight.
- 3Joint Stabilization WindowRestoring optimal scapular upward rotation requires 4 to 6 weeks of targeted serratus anterior strengthening.
- 4Return-to-Serve TimelineSymmetric rotator cuff strength of 90% compared to the uninjured side is required before resuming serving.
The Clinical Opinion: Dynamic Scapular Control vs. Passive Rest
"Treating rotator cuff tendinopathy in an elite tennis player requires active scapular re-education, not just resting the arm. In my clinical opinion, passive recovery allows the serratus anterior and lower trapezius muscles to weaken further, worsening impingement once the athlete plays again. By introducing progressive scapular stabilization drills early, we keep the shoulder blade moving correctly and relieve tendon compression."
Passive treatments fail to address the movement faults that cause tendon irritation. Resting the arm reduces acute pain, but the underlying scapular weakness remains, leading to immediate pain once the athlete resumes serving. Active scapular re-education is the key to achieving long-term shoulder safety.
Rehab begins with targeted strengthening of the serratus anterior and lower trapezius, which upwardly rotate the scapula. As muscle control improves, we introduce progressive rotator cuff strengthening, focusing on eccentric external rotation. This active reconditioning restores the shoulder's natural movement patterns, protecting the tendons from impingement.
Multi-Stage Rotator Cuff and Scapular Rehabilitation Protocol
Reconditioning an athlete's shoulder requires a progressive program that restores tendon strength, scapular coordination, and kinetic chain power.
Phase 1: Subacromial Decompression and Isometric Activation (Weeks 1-2)
The early phase focuses on reducing inflammation, protecting the healing tendons, and restoring passive range of motion. The athlete avoids overhead serving and high-impact loading. Manual therapy is performed to address posterior shoulder capsule tightness.
Sub-maximal isometric external rotation holds are performed to maintain rotator cuff activation without joint irritation. The athlete stands with their elbow bent to 90 degrees and presses the back of their hand against a wall, holding for 5 seconds. This exercise is performed in 3 sets of 10 repetitions twice daily.
Scapular retraction and depression exercises, such as wall slides and scapular squeezes, are introduced. These gentle movements engage the lower trapezius and serratus anterior. Restoring basic muscle activation lays the foundation for optimal scapular movement.
Phase 2: Scapular Upward Rotation and Eccentric Strengthening (Weeks 3-5)
Once isometric exercises are pain-free, we progress to active concentric and eccentric movements. The athlete performs eccentric external rotation exercises using a light resistance band, focusing on a slow, controlled release over a 4-second count.
Serratus anterior strengthening is progressed to push-up plus variations and dumbbell protractions. These exercises train the muscle to pull the shoulder blade forward and upward, maintaining the subacromial space. This targeted training is performed three times weekly.
Kinetic chain integration begins with squat-to-row exercises. The athlete performs a squat and uses the upward momentum to assist a resistance band row, engaging the legs, core, and shoulder. This whole-body coordination reduces the isolated load on the arm.
Phase 3: High-Velocity Deceleration and Sports-Specific Conditioning (Weeks 6-8)
The final phase focuses on rebuilding explosive rotator cuff deceleration power and tennis-specific speed. The athlete begins light plyometric training, performing medicine ball chest passes and overhead throws. These exercises train the muscles to absorb and redirect force.
Progressive serve reconditioning begins with shadow swings, focusing on proper kinetic chain sequencing. The athlete then progresses to light hitting, starting at 50% velocity and gradually increasing as tolerated. We monitor the shoulder closely for any post-exercise soreness.
High-velocity serving and match-play drills are introduced. Practicing serves from various court positions tests dynamic joint stability. These drills ensure the shoulder is ready to absorb the high-speed forces of competitive play.
Preventing Upper Body Kinetic Chain Compensations
A rotator cuff injury is deeply connected to neck and thoracic spine mechanics. Restricted thoracic mobility limits spinal extension during the serve wind-up, forcing the shoulder to hyperextend to compensate. This compensation increases the shear stress on the rotator cuff tendons.
To prevent secondary neck and upper back issues, the program incorporates thoracic mobility exercises and deep neck flexor strengthening. Ensuring optimal spinal alignment allows the shoulder blade to glide smoothly. A comprehensive approach is the key to maintaining long-term athletic health.
For more upper extremity rehabilitation guidelines, read our detailed guides on rotator cuff eccentric strengthening, scapular humeral rhythm in shoulder impingement, and thoracic mobility for shoulder relief. To understand sports-specific shoulder and wrist mechanics, view our analyses of Shohei Ohtani's shoulder subluxation, Jude Bellingham's shoulder subluxation, and Emma Raducanu's wrist surgery grip torque recovery. You can also review Ryan Jeffers' hamate fracture wrist rehabilitation.
Featured image attribution: Left panel displays tennis player Coco Gauff executing a serve. Right panel shows a clinical 3D medical illustration highlighting the shoulder joint, rotator cuff tendons, and local impingement points. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
