"Explosive power requires a tendon that acts like a steel spring, but when age-related stiffness meets a sudden, maximum stretch, even the strongest anatomical spring can snap under the pressure."
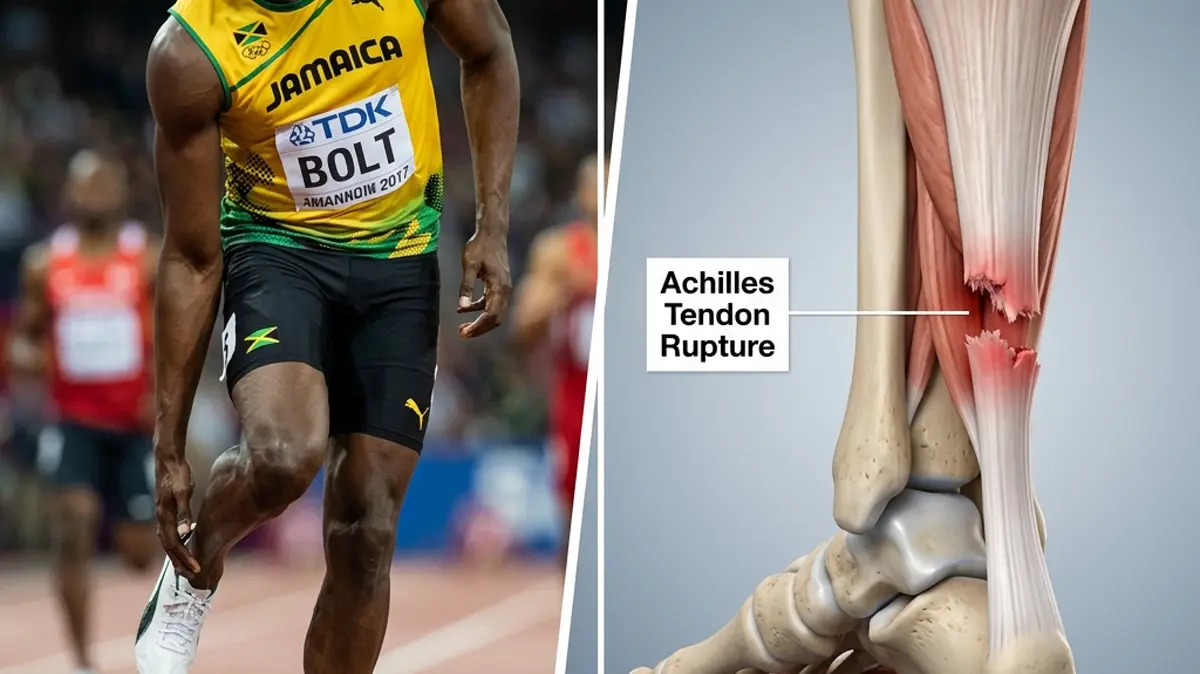
Usain Bolt's legendary sprint velocity and massive stride length redefined track and field athletics. However, generating that level of propulsion requires extreme mechanical force from the lower leg. When the world's fastest man sustains a complete Achilles tendon rupture, it highlights the extreme physical limits placed on the human ankle during high-velocity acceleration.
Many mature athletes view tendon stiffness as a normal part of aging, pushing through pain with supports and stretching. In reality, chronic tendon degeneration combined with high-load sports is a prime setup for a complete rupture. Rebuilding a ruptured tendon demands a structured post-surgical recovery program that emphasizes progressive mechanical loading.
Restoring elite sprinting performance requires understanding the biomechanics of tendon failure. By studying tissue remodeling rates and utilizing targeted usain bolt injury rehabilitation protocols, we can rebuild ankle power. This article examines the mechanics of Achilles trauma, surgical recovery phases, and progressive tendon loading.
The Biomechanics of Sprint Acceleration and Achilles Tendon Rupture
The Achilles tendon is the thickest and strongest tendon in the human body, transmitting forces up to twelve times body weight during sprinting. During the early acceleration phase, the calf muscles (gastrocnemius and soleus) contract dynamically while the ankle is forced into dorsiflexion (upward bending) as the foot strikes the ground. This creates a massive eccentric load on the tendon.
Immediately following this stretch, the tendon releases stored elastic energy in a powerful concentric recoil, driving the athlete forward. This rapid stretch-shortening cycle places immense tensile stress on the collagen fibers. If the tendon has pre-existing micro-damage or age-related vascular decline, this high-energy loading can exceed its structural limit, resulting in a sudden, painful rupture.
A rupture typically occurs 2 to 6 centimeters above the heel insertion, a region known as the watershed zone due to its poor blood supply. Following surgical repair, where the torn ends are sutured back together, the healing tendon is highly vulnerable. Without controlled loading, it heals with disorganized scar tissue that is stiff, weak, and prone to re-rupture.
Key clinical parameters for assessing Achilles tendon loading and recovery:
- 1Tensile Stress LoadDuring sprinting, the Achilles tendon absorbs loads equivalent to 12.5 times the athlete's body weight.
- 2Vascular DeclineTendon capillary blood flow drops by up to 40% between the ages of 25 and 40, slowing healing.
- 3Re-rupture Risk FactorEarly weight-bearing combined with orthotic heel lifts reduces the re-rupture rate to less than 3%.
- 4Limb Symmetry TargetAthletes require a 95% calf endurance symmetry before returning to high-velocity sprinting.
The Clinical Opinion: Early Mobilization vs. Prolonged Casting
"Rehabilitating a ruptured Achilles tendon in an elite sprinter requires early, controlled weight-bearing rather than months of plaster casting. In my clinical opinion, casting the foot in a pointed position for six weeks causes severe calf atrophy and permanent tendon shortening. By introducing gentle weight-bearing in a boot with heel wedges by week two, we stimulate collagen alignment and preserve muscle volume, speed-tracking athletic recovery."
Traditional recovery protocols kept the ankle immobilized in a cast for up to eight weeks, leaving the leg weak and stiff. Modern physical therapy instead utilizes early functional mobilization in a protective boot. Heel wedges are used to keep the ankle slightly pointed, reducing tension on the repaired tendon while allowing the athlete to walk.
Walking stimulates local circulation, which is vital for delivering nutrients to the healing watershed zone. As the tendon heals, wedges are gradually removed to restore normal ankle range of motion. Once the boot is removed, progressive loading is introduced to restore calf muscle strength and tendon elasticity.
Multi-Stage Post-Surgical Achilles Rehabilitation Protocol
Reconditioning a sprinter's ankle requires a systematic progression that builds tendon stiffness while restoring explosive power.
Phase 1: Protection and Controlled Weight-Bearing (Weeks 1-4)
The primary focus is on protecting the surgical repair and initiating weight-bearing. The athlete wears a protective boot with 3 heel wedges (placing the ankle in 30 degrees of plantarflexion). The athlete is allowed to bear weight as tolerated using crutches.
Passive ankle movements are performed only in the direction of pointing the foot (plantarflexion) to prevent calf contracture. Active dorsiflexion past neutral is strictly avoided to protect the repair from stretching. Swelling is managed with daily compression and elevation.
Core, hip, and upper body conditioning are maintained to prevent overall fitness loss. The athlete performs seated upper body drills and core exercises that do not put pressure on the ankle.
Phase 2: Boot Removal and Progressive Loading (Weeks 5-12)
Around week 6-8, the boot is removed, and the athlete transitions to normal athletic shoes with a small silicone heel lift. Rehabilitation focuses on restoring normal walking gait and introducing active ankle strengthening.
We initiate seated calf raises, gradually progressing to standing double-leg heel raises. The athlete performs these exercises slowly, focusing on a 3-second raise and a 3-second descent. This controlled loading stimulates tendon repair without excessive stretch.
Single-leg balance exercises are introduced to rebuild ankle proprioception. The athlete stands on the injured leg on a flat surface, gradually progressing to unstable surfaces like foam pads as balance improves.
Phase 3: Eccentric Power and Sprint Reconditioning (Months 4-9)
The final phase focuses on restoring high-velocity tendon stiffness and sprinting power. The athlete performs heavy-resistance eccentric calf raises, lowering the heel below the step level. This builds tissue tolerance under stretch.
Plyometric drills begin with double-leg hopping and advance to single-leg bounds. These dynamic movements train the tendon to store and release elastic energy. Ankle range of motion is monitored closely to ensure optimal joint mobility.
Running progression begins on a linear track, starting with low-intensity jogging and advancing to acceleration drills. The athlete returns to competitive sprinting only after achieving symmetrical calf strength and passing sport-specific speed tests.
Securing the Kinetic Chain
An Achilles tendon rupture is a severe injury that places stress on the entire leg. Weakness in the calf muscles forces the knee and hip to compensate, leading to altered gait mechanics. Prolonged limping can strain the lower back and contralateral leg, causing secondary pain.
To prevent these issues, the rehabilitation program must target the entire kinetic chain. Strengthening the gluteal muscles and maintaining hip mobility ensures that weight is distributed evenly across both legs. A balanced kinetic chain is the foundation for a successful return to sport.
To learn more about lower extremity rehabilitation, read our detailed guides on Achilles tendinitis HSR protocols, ankle sprain joint stability, and plantar fasciitis posterior chain release. You can also view our athletic analyses of Kevin Durant's Achilles recovery, Aaron Rodgers' speed-healing biomechanics, and Usain Bolt's scoliosis and hamstring biomechanics.
Featured image attribution: Left panel displays a visual representation of sprinter Usain Bolt showing heel pain during a race. Right panel shows a detailed 3D medical anatomical illustration highlighting the gastrocnemius muscle, soleus muscle, and a ruptured Achilles tendon above the calcaneus bone. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
