"A modern topspin forehand is a masterpiece of kinetic energy, but when the wrist snap overrides the support of the forearm muscles, the pronator teres is forced to absorb a structural breaking load."
Carlos Alcaraz's aggressive baseline play and explosive forehand make him one of tennis's most thrilling stars. However, generating extreme racquet head speed requires immense muscular control. When a player of his caliber suffers a forearm strain, it highlights the heavy mechanical toll modern baseline tennis exacts on the elbow and wrist.
Many tennis players treat forearm pain as a minor issue, playing through it with tape and anti-inflammatories. In reality, ignoring localized forearm soreness leads to micro-tearing at the muscle-tendon junction. Rebuilding a durable forearm requires correcting the mechanical forces acting on the flexor-pronator mass.
Restoring elite tennis performance demands analyzing the biomechanics of forehand acceleration. By studying grip alignment and utilizing targeted carlos alcaraz injury rehab protocols, we can restore joint stability. This article breaks down pronator teres biomechanics, rehabilitation stages, and modern tennis reconditioning.
The Biomechanics of Topspin Forehands and Pronator Teres Overload
The modern topspin forehand relies on a biomechanical chain that starts at the feet and ends with a whip-like snap of the wrist. To generate massive topspin, elite players use a semi-western or western grip. This grip forces the forearm into a highly pronated and flexed position at ball contact, overloading the muscles on the inside of the elbow.
During the acceleration phase of a forehand, the racquet lag puts the forearm flexors on a massive eccentric stretch. At ball contact, the player violently pronates the forearm and snaps the wrist forward to pull the racquet over the ball. This rapid transition from eccentric stretch to concentric contraction creates immense mechanical tension on the pronator teres.
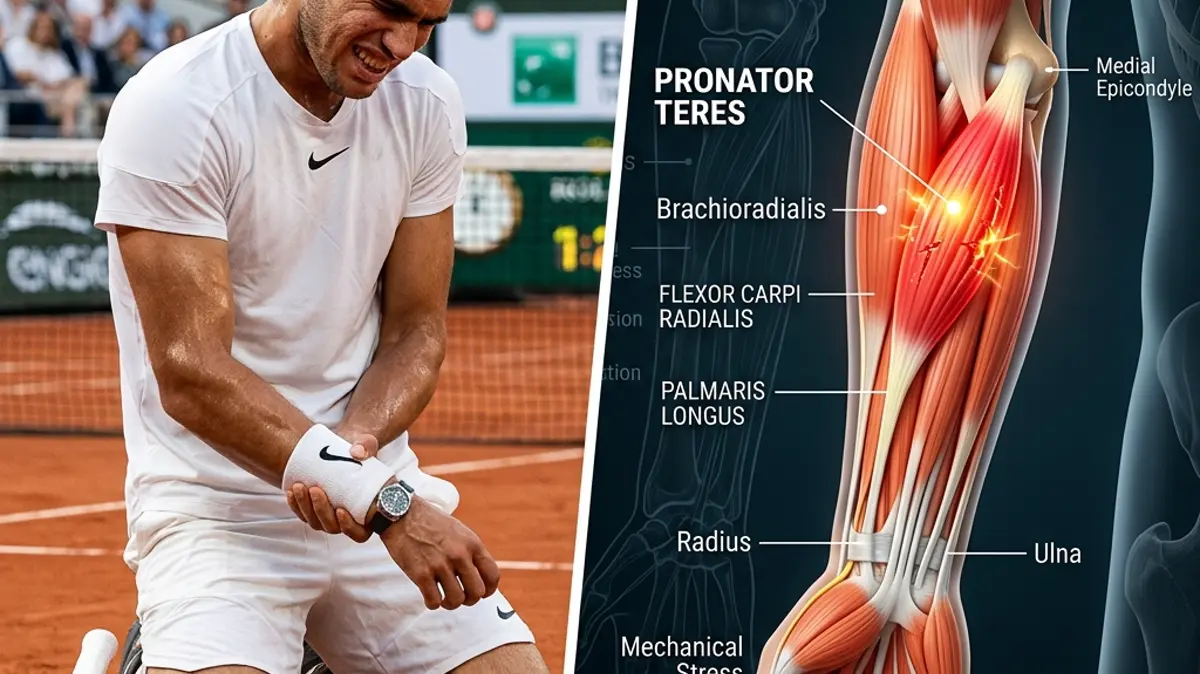
If the wrist stabilizers are fatigued, the pronator teres is forced to absorb the excess rotational torque. Over time, this repetitive loading leads to microscopic muscle fiber tearing, particularly near the medial epicondyle attachment. Compensatory tension quickly spreads up the arm, straining the shoulder and scapular stabilizers.
Key clinical parameters for assessing pronator teres strain and recovery:
- 1Rotational LoadModern forehands subject the forearm to rotational velocities exceeding 1500 degrees per second.
- 2Grip Force ImpactAn unbalanced semi-western grip spikes the mechanical shear force on the medial epicondyle by 35%.
- 3Tissue Repair TimelineControlled eccentric wrist flexion must begin by day 10 to guide parallel collagen remodeling.
- 4Return-to-Play ThresholdAthletes must achieve a 90% grip strength symmetry to clear dynamic baseline tennis play.
The Clinical Opinion: Load Adaptation vs. Complete Immobilization
"Treating a pronator teres strain in a high-velocity tennis player requires active load management rather than complete wrist immobilization. In my clinical opinion, placing the arm in a rigid splint causes rapid muscular atrophy and worsens tendon stiffness. By introducing pain-free isometric pronation holds early, we preserve neuromuscular pathways and guide healthy tissue healing, preventing chronic reinjury."
Standard sports medicine often prescribes absolute rest and brace wear for forearm pain. While immobilization reduces acute discomfort, it leaves the muscle weak and prone to re-injury. Modern physical therapy instead utilizes progressive mechanical loading to stimulate tissue adaptation.
Early isometric activation improves localized circulation and helps align new collagen fibers along their natural axis. As pain subsides, we gradually introduce eccentric training to strengthen the tissue during lengthening. This eccentric capacity is crucial for absorbing the violent decelerating forces of tennis swings.
Multi-Stage Forearm and Wrist Pronation Rehabilitation Protocol
Reconditioning a tennis player's forearm requires a systematic progression that builds tissue tolerance while restoring grip and wrist coordination.
Phase 1: Protection and Isometric Activation (Weeks 1-2)
The primary goal is to protect the healing muscle fibers and manage inflammation without causing joint stiffness. The athlete avoids heavy gripping, serving, and topspin forehands. Cryotherapy and myofascial release are used to reduce localized muscle guarding.
We introduce sub-maximal isometric pronation exercises. The athlete holds a hammer by the shaft, forearm supported on a table, and gently resists rotational forces for 10 seconds. This exercise is performed in 3 sets of 10 repetitions twice daily.
Wrist extension stretches and passive wrist flexor mobility are maintained to keep the tissue long. The athlete maintains neutral wrist alignment during daily activities to avoid overloading the medial flexor-pronator mass.
Phase 2: Concentric Loading and Grip Integration (Weeks 3-4)
Once pain-free rotation is achieved, active concentric movements are introduced. The athlete performs light dumbbell wrist curls and forearm pronation exercises through a comfortable range of motion. Resistance is kept light, focusing on perfect alignment.
We integrate grip-strengthening exercises to rebuild the dynamic support of the hand. The athlete performs grip-squeeze holds using a soft foam ball or putty, maintaining a neutral wrist position. This balances the flexor tendons and reduces strain on the pronator teres.
Controlled eccentric loading begins with slow wrist extension-to-flexion movements. The athlete lifts a light dumbbell with the opposite hand and slowly lowers it over 5 seconds. This prepares the tissue for tennis impact forces.
Phase 3: Eccentric Power and Court-Specific Reconditioning (Weeks 5-8)
The final phase focuses on high-velocity eccentric strength and tennis-specific movement patterns. The athlete performs heavy-resistance forearm pronation drills and dynamic wrist extension holds. These drills train the forearm to handle sudden deceleration.
Racquet training begins on the court, starting with light mini-tennis volleys at 40% intensity. The athlete avoids hitting heavy topspin forehands and kick serves in the initial sessions. Velocity is increased by 10% each session as tolerated.
Full-baseline drilling and match play are introduced once grip strength and endurance are symmetrical. We monitor the forearm for any post-session stiffness, using post-play stretching to maintain muscle length.
Preventing Kinetic Chain Overloads in Tennis
Forearm injuries rarely occur in isolation; they are deeply connected to the biomechanics of the shoulder and spine. Weakness in the rotator cuff or scapular stabilizers forces the wrist and forearm to work harder to generate power. This compensation quickly overloads the smaller muscles of the forearm.
To ensure long-term elbow and wrist health, a complete rehabilitation program must address the entire kinetic chain. Strengthening the upper back and core ensures that force is generated from the larger muscle groups of the body. A balanced kinetic chain is the ultimate safeguard for a high-performance athlete.
To learn more about upper extremity recovery, read our detailed guides on carpal tunnel wrist ergonomics, rotator cuff eccentric strengthening, and medial epicondylitis recovery protocols. You can also review our biomechanical analyses of Emma Raducanu's wrist surgery recovery, Coco Gauff's rotator cuff tendinopathy, and Shohei Ohtani's shoulder subluxation biomechanics.
Featured image attribution: Left panel displays a visual representation of tennis player Carlos Alcaraz on court showing forearm discomfort. Right panel shows a detailed 3D medical anatomical illustration highlighting the flexor-pronator mass and pronator teres muscle structure of the forearm. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
