Anterior Pelvic Tilt Exercises: 3-Step Fix & Daily Tracker
"Anterior pelvic tilt is not a static disease to be cured. It is a dynamic movement pattern. Train your nervous system to stabilize the pelvis during motion, and the static posture will take care of itself."
You have likely spent months stretching your hip flexors and doing glute bridges. Yet, every time you stand in front of the mirror, your lower back still curves like an overripe banana and your abdomen protrudes forward. You might feel like your body is permanently stuck in a structural dent.
The fault is not your effort — it is the strategy. Trying to force a static pelvic correction by just aggressively stretching is like trying to align your car's steering wheel by polishing the dashboard. The pelvis is a three-dimensional ring controlled by ten muscle groups, not a simple hinge.
To finally get results, you need a structured, active anterior pelvic tilt exercise protocol. This guide outlines the exact three-phase system designed to build real pelvic motor control.
The Myth of the \"Pathological\" Tilted Pelvis
Before diving into exercises, we must address the single biggest misconception in the fitness industry. Many online sources treat anterior pelvic tilt (APT) as a dangerous abnormality that causes herniated discs and chronic joint degeneration. This is simply not supported by modern biomechanical research.
Clinical studies show that 75% to 85% of healthy, completely pain-free adults naturally present with an anterior pelvic tilt. It is a normal anatomical variation, much like being left-handed or having flat feet. If you do not have lower back pain or hip pinches, your pelvic tilt is likely just how your skeleton is built.
However, if you do experience symptoms like lower back stiffness after standing, or a pinching feeling in the front of your hip during deep squats, then active management is warranted. The focus should never be on achieving a "perfectly straight" pelvis, but rather on building dynamic control and shock absorption.
The Real Biomechanics of Anterior Pelvic Tilt
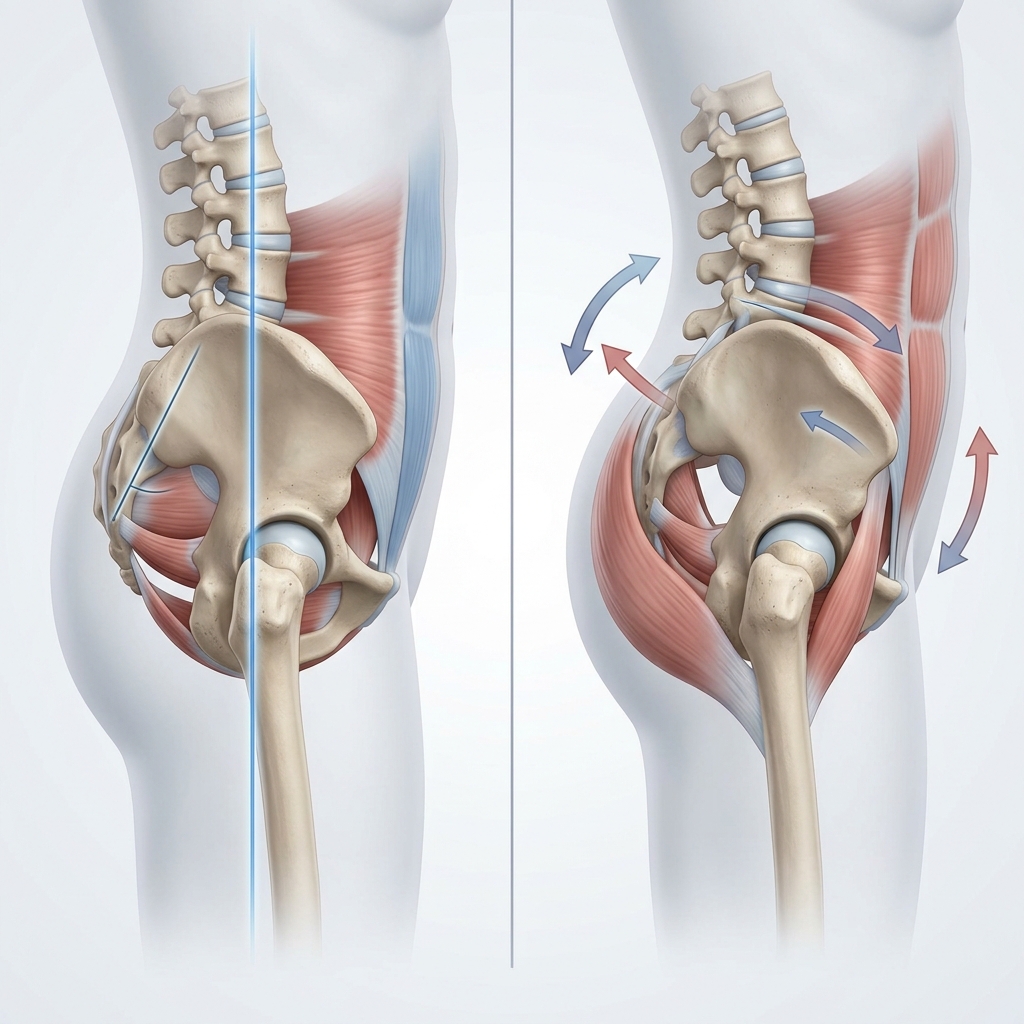
Anterior pelvic tilt occurs when the front of your pelvis rotates downward while the back rises. Think of your pelvis as a bucket of water: in an anterior tilt, the bucket tips forward and water spills out the front. This forces your lumbar spine to arch excessively, a state known as lumbar hyperlordosis.
While a mild tilt is normal, an excessive tilt shifts static mechanical load away from your muscles and directly onto your lumbar facet joints. The clinical threshold for a significant tilt is an angle exceeding 10 degrees in men and 13 degrees in women. At these positions, lumbar disc compressive forces increase by up to 35%, and the surrounding tissues must work twice as hard to stabilize you.
An excessive tilt is governed by a classic cross-pattern muscle imbalance around the pelvic ring:
- 1Overactive Front Hip FlexorsThe iliopsoas and rectus femoris are chronically shortened from prolonged sitting, pulling the front of your pelvis down.
- 2Overactive Lower Back ExtensorsThe erector spinae muscles tighten to support the arch, acting as a rigid pulley pulling the back of the pelvis upward.
- 3Inhibited Gluteal ComplexThe gluteus maximus is the body's primary posterior pelvic rotator. Sitting for hours causes "gluteal amnesia," turning off these essential anchors.
- 4Weak Deep AbdominalsThe rectus abdominis and obliques are responsible for pulling the front pelvis upward. Without their counter-tension, the pelvis rotates unchecked.
The Clinical Opinion: Stop Passive Hip Flexor Stretching First
"The most common mistake patients make is leading their rehabilitation with aggressive, passive hip flexor lunges. A tight hip flexor is like a protective bouncier outside a VIP club; it is tight because your core is unstable. If you stretch it without building abdominal stability first, your nervous system will sense the instability and clamp the muscle back down tighter within twenty minutes."
Start Your Daily Interactive Posture Tracker
To help you stay consistent, we have built a gamified tracker directly into this guide. Settle into a routine, check off your daily exercises, and track your recovery streak to build lasting habits.
The Correct 3-Step Pelvic Tilting Exercise Protocol
To reprogram your posture, you must train your brain and muscles to communicate. Focus on the quality of muscle contractions rather than rushing through the movements.
Phase 1: Neuromuscular Coordination
Before you can strengthen, you must teach your brain how to move the pelvis. The supine posterior pelvic tilt is the foundation of this phase. Lie on your back with your knees bent and feet flat on the floor. Draw your lower stomach inward, then contract your glutes and abdominals to flatten your lower back completely against the floor. Hold this contraction for 5 seconds, breathing normally, then relax. Perform 3 sets of 12 repetitions daily.
Phase 2: Core and Hip Co-Stabilization
Once you can tilt your pelvis, you must learn to hold that position under load. The gold standard for this is the dead bug exercise. Lie on your back, raise your legs to a tabletop position (90-degree bend), and extend your arms toward the ceiling. Perform a posterior pelvic tilt to lock your lower back against the floor. Slowly lower your right arm and left leg toward the floor, maintaining a completely flat lower back. If your back arches, you have exceeded your core capacity. Return to the starting position and repeat on the other side, aiming for 3 sets of 8 reps per side.
Phase 3: Active Hip Mobilization
Only after establishing core stability should you stretch the hip flexors. To perform the active kneeling hip flexor stretch, step into a half-kneeling position. Squeeze the glute of your trailing leg as hard as you can to tilt your pelvis backward. Keeping your torso upright, gently shift your weight forward. You should feel a deep, localized stretch in the front of your thigh. Hold for 30 seconds, repeating 2 times on each side.
The Patient: Marcus, a 31-year-old software engineer, suffered from chronic lower back tightness after sitting 10+ hours a day. He had a prominent pelvic tilt and arch.
The Mistake: He spent four months performing aggressive runner's lunges and hamstring stretches daily. His back pain actually got worse because he was arching into the stretches.
The Solution: We stopped all passive stretching for two weeks. He focused entirely on supine pelvic tilts, dead bugs, and active glute bridging. Once his core stability improved, we introduced active kneeling stretches.
The Outcome: Marcus reported an 85% reduction in lower back stiffness within 6 weeks. His pelvic inclination angle normalized, and he can now sit comfortably throughout his workday.
Integrating Pelvic Tilts Into Your Workday
Reprogramming your nervous system requires consistent feedback. Performing exercises on a yoga mat is not enough if you slouch at your desk for the remaining 23 hours of the day. Perform a quick pelvic check every time you stand up from your chair. Squeeze your glutes, tuck your tailbone slightly, and hold for two seconds. This simple micro-habit will build structural resilience faster than any passive therapy.
For complementary recovery guides, read our clinical breakdown of core stability exercises and our guide on SI joint dysfunction stabilization. If you want to strengthen your deep abdominal corset, see our article on transversus abdominis activation to protect your lower back from daily mechanical shear.
Featured image: Medical illustration demonstrating correct pelvic tilting exercise alignment. Prepared for AyurPhysio clinical reference.
Irushi Abeywardhana
Senior Physiotherapist & Founder of Physio Pulse. Senior Clinical Physiotherapist passionate about blending advanced movement science with functional resilience.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →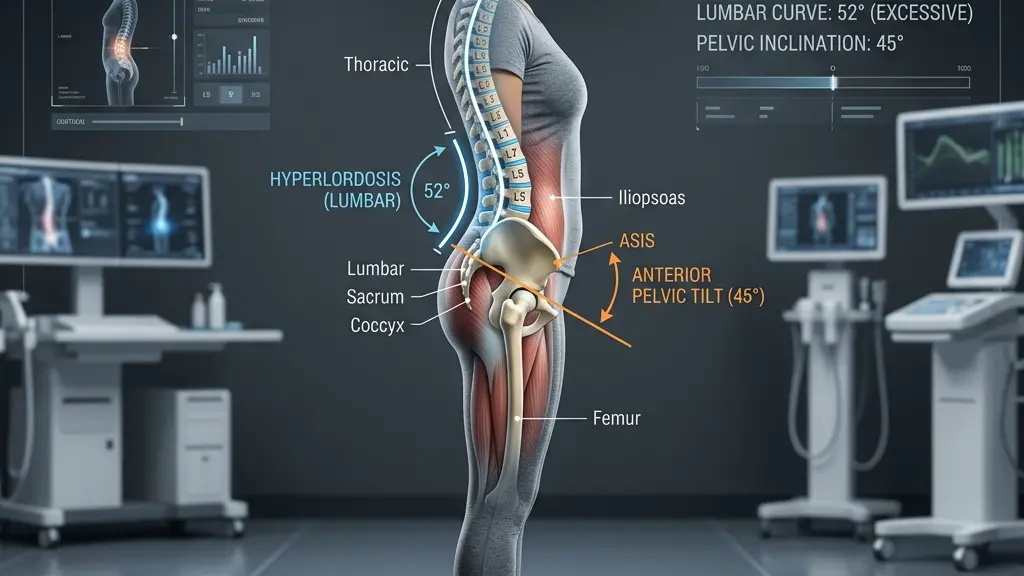
Hyperlordosis: Tailoring Exercise Programs to Reduce Lumbar Shear Stress

Morning Lower Back Stiffness: The Biomechanical Causes and Quick, Safe Fixes
