Sciatica vs. Piriformis Syndrome: The Clinical Differences in Diagnosis
"If sciatica from a herniated disc is a kink in the hose at the main faucet in your spine, piriformis syndrome is someone stepping on that same hose halfway down your garden path in the glutes."
Waking up with a sudden bolt of electricity radiating down your leg is one of the most terrifying structural sensations you can experience. The pain starts deep in your hip and races down to your calf, leaving you unable to stand straight, walk comfortably, or sit down at your desk.
Most individuals who experience this sharp, shooting sensation immediately jump to the worst-case scenario. They assume they have a severe ruptured disc, spiral into anxiety over potential spinal surgery, and immediately look up lower back nerve pain treatments online.
But here is the clinical reality: not all shooting leg pain originates in your spine. In fact, an often-overlooked muscle deep in your buttocks might be the true culprit behind your agony, mimicking spinal pathology while keeping your lower back perfectly healthy.
Understanding the critical anatomical differences between true sciatica and its structural mimic is the absolute first step toward finding permanent, targeted shooting leg pain relief.
The Anatomy of the Fake-Out: Nerve vs. Muscle
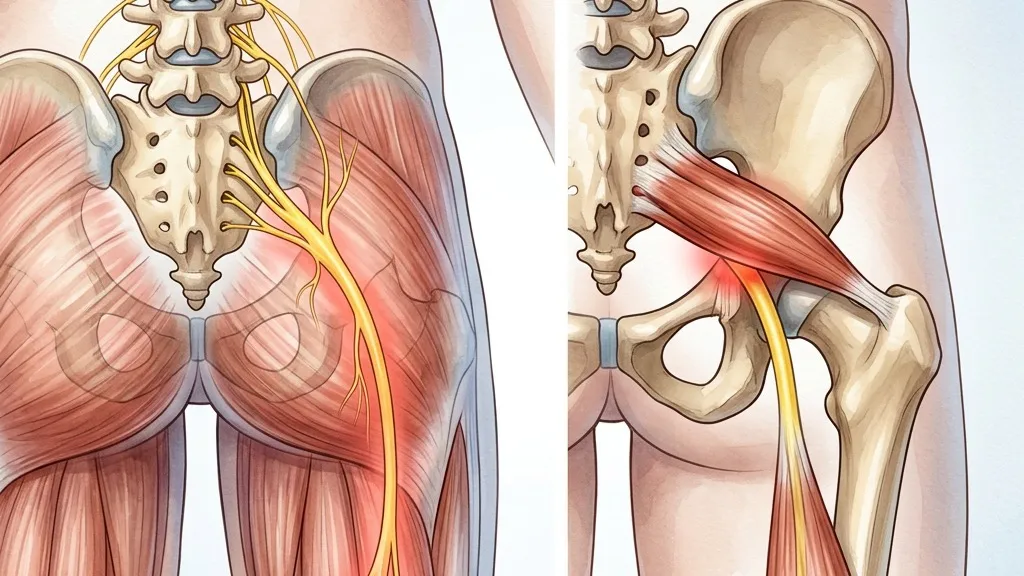
The sciatic nerve is the longest and thickest nerve in the human body, measuring roughly the width of your thumb. It begins in your lower lumbar spine, travels through the gluteal region, and runs all the way down to the tips of your toes.
In true sciatica, the source of your pain is located at the spine itself. This is typically caused by a lumbar disc bulging outward and physically compressing the nerve root at the exit canal.
Piriformis syndrome, however, occurs further down the line. The piriformis is a flat, band-like muscle that stabilizes the hip joint. In roughly 15% of the population, the sciatic nerve actually passes directly through the belly of this muscle instead of underneath it.
Clinical studies reveal that approximately 6% of patients diagnosed with sciatica actually suffer from localized piriformis syndrome. This causes thousands of patients to undergo unnecessary lumbar spinal injections or targeted spinal traction routines for an issue that exists exclusively in their gluteal muscles.
Furthermore, clinical research demonstrates that a standard Straight Leg Raise (SLR) test has an astonishing 91% sensitivity rate for detecting lumbar disc herniations. If you cannot lift your leg past 45 degrees while lying flat, your spine is likely involved.
Conversely, if your pain is aggravated by crossing your legs while sitting, or by performing a FAIR (Flexion, Adduction, Internal Rotation) maneuver, the compression is localized in your hip rotators.
Why Stretching Your Spine is Making Your Buttock Pain Worse
When people experience shooting leg pain, they often perform aggressive lumbar flexion stretches like pulling their knees to their chest. They believe that by round-stretching their back, they are opening up their spinal discs.
My authoritative clinical insight as a lead therapist is that blindly executing lumbar flexion stretches without confirming your specific diagnosis is a recipe for prolonged neurological inflammation. If you are dealing with true discogenic sciatica, bending your spine forward pushes your disc material further backward, spiking your intradiscal pressure to over 180% and intensifying the nerve compression.
Conversely, if your issue is piriformis syndrome, aggressive hamstring and glute stretches can over-sensitize a nerve that is already chemically inflamed. To heal permanently, you must move beyond generic stretches and actively implement sciatic nerve mobilization designed for your unique pathology.
Understanding the mechanics of why your back aches after sitting can offer critical insights into whether your posture is driving spinal compression or gluteal tightness.
The Patient: Marcus, a 42-year-old software engineer and marathon runner, suffered from constant, burning pain down his left hamstring that forced him to stop running entirely.
The Mistake: Assuming a herniated disc, Marcus spent two months doing lumbar extension exercises and core bracing, which did absolutely nothing to relieve his burning thigh pain.
The Solution: Our assessment revealed negative spinal signs but severe tenderness directly over his piriformis muscle. We shifted his treatment to progressive hip abductor strengthening and localized sciatic nerve gliding.
The Outcome: Within 4 weeks of targeted gluteal therapy, his leg pain vanished entirely. By week 8, Marcus returned to running 15 miles a week with absolute biomechanical comfort.
Three Clinical Steps for Targeted Relief and Correction
To successfully differentiate and manage your symptoms, you must establish a solid routine built around structural stability. Start by building a foundation of robust core stability, then perform these specific actions:
-
1The FAIR Maneuver Test (Diagnostic Screen) Lie on your side with your painful leg on top. Bend your top hip and knee to 90 degrees, then gently pull your knee down toward the table to internally rotate your hip. If this reproduces your deep shooting pain in the buttock, you likely have a positive piriformis syndrome diagnosis, and should focus on gluteal release rather than spinal manipulation.
-
2Active Sciatic Nerve Flossing (Neural Mobility) Sit tall in a chair. Straighten your painful knee while simultaneously looking up at the ceiling. Then, lower your leg back down while simultaneously looking down at your chest. Perform 15 slow, rhythmic repetitions. This "flosses" the nerve back and forth through the piriformis and spinal canals, reducing adhesion without tensioning the nerve.
-
3Hip Abductor Stability (Clamshell Progressions) Lie on your side with both knees bent and an elastic band around your knees. Keeping your heels pressed together, open your top knee slowly, ensuring your pelvis does not roll backward. Perform 3 sets of 12. Strengthening your outer hips removes the load from your overactive piriformis, providing permanent, long-term joint protection.
Take Targeted Action for Your Nerve Health
Your body's nervous system is highly sensitive, but it responds beautifully to precise, mechanical corrections. By understanding the exact source of your neurological symptoms and discarding generic advice, you can successfully break the pain cycle. Are you ready to stop guessing and start addressing the true mechanical engine of your discomfort today?
Irushi Abeywardhana
Senior Physiotherapist & Founder of Physio Pulse. Senior Clinical Physiotherapist passionate about blending advanced movement science with functional resilience.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →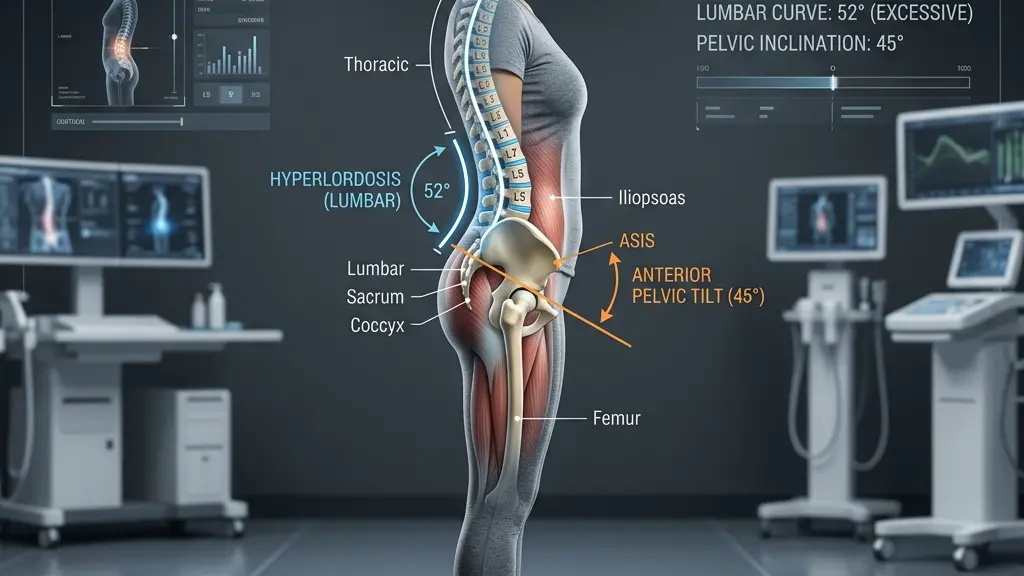
Hyperlordosis: Tailoring Exercise Programs to Reduce Lumbar Shear Stress

Morning Lower Back Stiffness: The Biomechanical Causes and Quick, Safe Fixes
