"A wrist hairline fracture is like a micro-crack in a high-performance frame. Under normal conditions, it looks completely stable, but if you subject it to a collision before repairing it, the entire structure can snap."
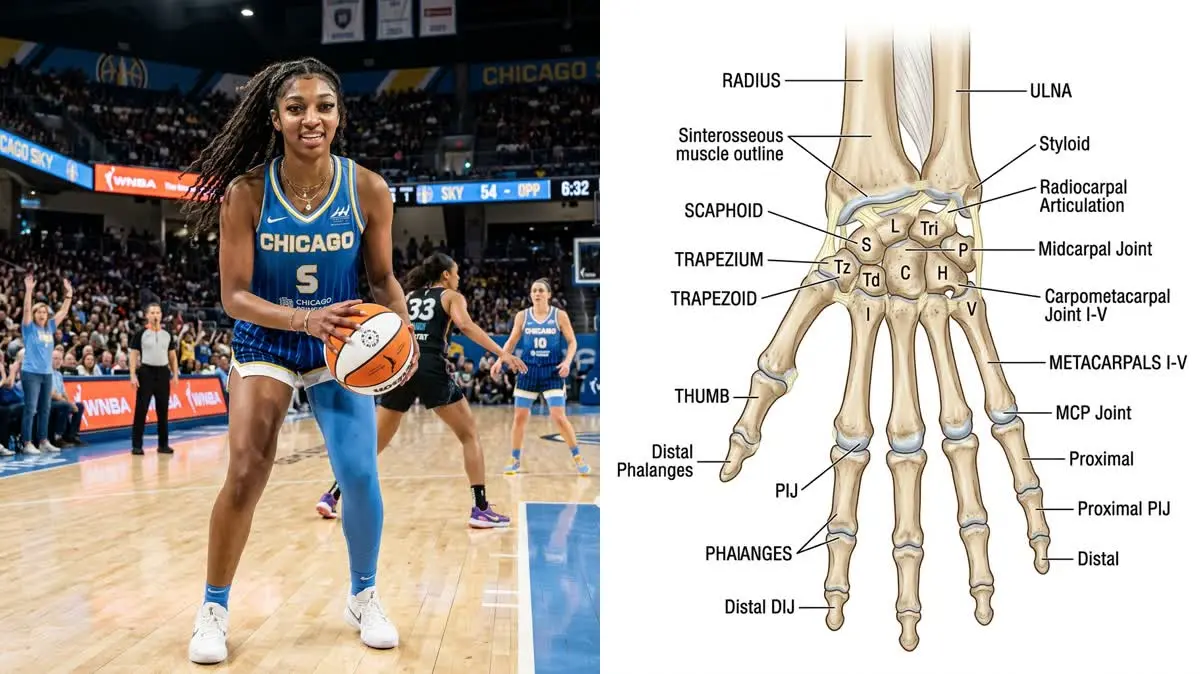
The season-ending hairline fracture in Angel Reese's left wrist cut short her historic rookie season with the Chicago Sky. For an elite basketball player whose game is built on aggressive physical play, wrist stability is a vital necessity. Restoring joint integrity is the primary focus of her athletic recovery.
Traditional treatments like casting often lead to joint stiffness and muscle wasting. For an elite athlete, prolonged rest is rarely the optimal path. Modern sports medicine utilizes precise loading to guide bone healing and maintain athletic conditioning.
Restoring WNBA-level ball-handling requires addressing the exact mechanics of the injury. By studying the forces acting on the joint and using targeted angel reese wrist fracture rehabilitation, we can rebuild a resilient hand.
This article reviews the biomechanics of wrist trauma, clinical decision-making, and a structured rehabilitation progression.
The Biomechanics of FOOSH and Hairline Trauma
A hairline wrist fracture typically occurs from falling on an outstretched hand (FOOSH). When an athlete lands and instinctively extends their arm, their entire body weight channels directly through the palm. This impact creates a sharp mechanical overload.
The force travels through the carpal bones to the distal radius and scaphoid. If this energy exceeds the bone's structural threshold, it creates a linear crack without displacement. High athletic acceleration makes the wrist highly vulnerable to these impact forces.
This fracture represents a disruption in the bone's trabecular architecture without cortical displacement. The sudden overload triggers a cellular inflammatory cascade to clear damaged matrix. Within days, osteoblasts recruit to lay down new osteoid tissue.
Distal radius fractures account for approximately 18% of all skeletal fractures. Furthermore, scaphoid and radius injuries make up 25% of sports-related hand trauma. Recovery requires protecting the healing bone while preventing surrounding tissues from tightening.
Basketball players must also absorb intense contact and rotational forces during play. A passing impact can generate compression forces three times the athlete's weight. Premature loading can displace a stable hairline crack, requiring surgical revision.
Key clinical parameters tracking bone healing and hand performance outcomes:
- 1Sports PrevalenceHand and wrist injuries account for up to 25% of all sports-related skeletal trauma.
- 2Grip Strength LossImmobilization of the wrist for over 4 weeks causes a 30% reduction in grip strength.
- 3Bone Healing WindowPrimary bone healing of a hairline fracture requires 6 to 8 weeks of controlled loading.
- 4Re-injury PreventionRestoring full wrist extension to 70 degrees is essential to safely absorb future landing impact.
The Clinical Opinion: Active Fixation vs. Passive Casting
"Following a non-displaced wrist fracture, the choice of treatment determines the athlete's recovery timeline. In my clinical opinion, percutaneous screw fixation is a game-changer because it provides immediate mechanical stability. This internal support allows us to start active mobility drills within the first post-operative week, preventing joint stiffness."
Professional sports rehabilitation aims to minimize joint immobilization. Passive casting for six weeks causes forearm muscle atrophy and capsular tightness. In contrast, surgical screw fixation provides rigid compression across the fracture line, allowing immediate mobility.
The screw acts as an internal splint to share the mechanical load and prevent micro-motion. This rigid stability allows physical therapists to introduce active range of motion early, preserving cartilage health. Maintaining joint mobility prevents chronic pain and contractures.
Multi-Stage Wrist and Hand Rehabilitation Protocol
Reconditioning a player's wrist requires a progressive approach that respects bone healing timelines while restoring the hand's kinetic chain.
Phase 1: Protection and Controlled Mobilization (Weeks 1-3)
The early phase focuses on controlling swelling, protecting the bone, and maintaining adjacent joint mobility. A custom-molded thermoplastic splint shields the wrist during daily tasks. Active finger movements are performed hourly to prevent tendon adhesion.
Active-assisted wrist extension and flexion are introduced within a pain-free 15-degree arc. We strictly avoid ulnar and radial deviation to prevent shear stress at the fracture site. Swelling is managed via compression wrapping and elevation.
Sub-maximal isometric contractions of the forearm musculature maintain muscle tone without joint movement. The athlete performs brief five-second holds against a solid barrier. This muscle activation enhances local circulation and stimulates early bone healing.
Phase 2: Progressive Strengthening and Joint Mobilization (Weeks 4-6)
Once bone healing is confirmed radiographically, we transition the athlete to active strengthening. Sub-maximal isometric holds are performed in flexion, extension, and pronation to re-engage the forearm. The athlete performs 3 sets of 10 repetitions.
We gradually introduce active stretches to restore the normal 70 degrees of extension. Passive joint mobilizations address capsular tightness in the radiocarpal joint. These targeted exercises are performed three times per week.
Resistance band exercises are added to build multi-directional wrist stability. The patient performs controlled movements against light resistance to strengthen the wrist stabilizers. This progressive loading prepares the joint for impact.
Phase 3: Grip Torque and Sports-Specific Conditioning (Weeks 7-10)
Phase three focuses on restoring maximum grip strength and basketball-specific impact tolerance. The athlete utilizes spring-loaded grippers to strengthen the intrinsic hand muscles. Forearm pronation and supination are rebuilt using weighted bar rotations.
Light handling drills begin with soft tennis ball catches before progressing to standard dribbling. We monitor the joint closely for post-exercise warmth or swelling. The athlete performs dynamic dribbling drills twice weekly.
The final stage involves high-velocity pass catching and rebound drills on the court. Practicing catches from various angles tests dynamic joint stability. These drills ensure the wrist is ready for live game forces.
Preventing Secondary Kinetic Chain Failures
A wrist injury is never isolated; immobilization affects the entire upper extremity kinetic chain. Wrist tightness leads to pronator teres spasm and supinator muscle weakness. This imbalance alters elbow loading, straining the medial collateral ligament.
The shoulder often compensates for lost mobility, causing upper trapezius dominance and scapular winging. To prevent secondary issues, the program includes scapular stabilization exercises. Chest presses and wall slides maintain full kinetic chain integration.
Addressing the entire limb ensures the athlete returns to play with balanced biomechanics. This holistic conditioning is the key to preventing secondary kinetic chain failures.
For more upper extremity recovery guidelines, read our detailed guide on nerve gliding and wrist ergonomics and view our breakdown of De Quervain's thumb tendonitis rehab. To understand sports-specific hand mechanics, check our analysis of catcher hand rehab following hamate fractures and wrist surgery grip torque recovery in tennis players. To learn about elite wrist loading, view our analysis of scapholunate ligament recovery in quarterbacks.
Featured image attribution: Left panel photo of Angel Reese adapted from Wikimedia Commons page (File:Angel Reese 2024.jpg). Right panel displays a clinical anatomical diagram of the wrist and hand bones. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
