"The Achilles tendon is like a heavy-duty industrial bungee cord. If you stretch and snap it, splicing the ends together makes it functional again, but if you don't rebuild its elasticity, the next high-speed jump will simply snap the cord at the splice point."
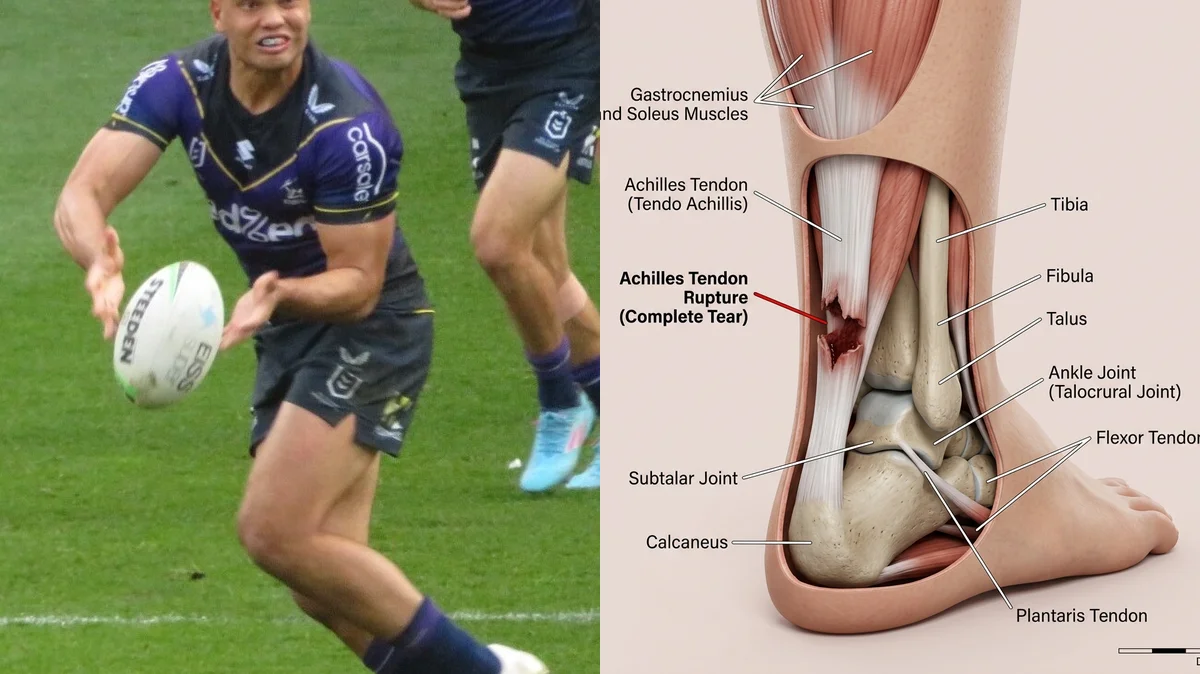
The news that Melbourne Storm and Queensland Maroons star winger Xavier Coates suffered a recurrent Achilles tendon rupture has raised serious concerns about his long-term playing career. For an elite rugby player dependent on high-speed chasing, sudden stops, and vertical jumping, this injury represents one of the most difficult challenges in sports rehab. When a previously repaired tendon ruptures again, the healing process is complicated by existing scar tissue and reduced blood flow.
Standard recovery protocols that focus solely on rest and passive stretching often fail to rebuild the tendon's stiffness, leaving the athlete vulnerable to future tears. A tendon that has been ruptured twice loses its natural elasticity and strength, requiring a highly structured, progressive loading program to rebuild the tissue. Without this targeted stimulation, returning to contact sports is highly risky.
To safely return to play and protect the joint from future injuries, we must focus on tissue loading and joint mechanics. Through a detailed analysis of the xavier coates achilles tendon rupture, we can develop a matching recovery plan. This guide examines the mechanics of recurrent achilles tendon rupture and details the clinical steps to rebuild calf and tendon function.
The Biomechanics of Recurrent Tendon Rupture
The Achilles tendon is the main spring of the lower leg, absorbing forces during landing and releasing energy during push-off. During high-impact movements, the tendon experiences loads up to 8 times body weight. When a player suffers a second rupture, the injury typically occurs at the boundary where the old scar tissue meets the healthy tendon, an area prone to stress concentrations.
Scar tissue is composed of disorganized Type III collagen, which is less elastic than the structured Type I collagen found in healthy tendons. This difference in flexibility means that when the tendon is stretched, the scar tissue cannot stretch as easily, placing excessive stress on the surrounding healthy tissue. This load difference, combined with altered ankle joint kinematics, is a major driver of recurrent injuries.
Clinical statistics show that the rate of recurrent Achilles tendon ruptures in professional athletes is approximately 5%, with the risk rising if calf strength is not fully restored. Concomitant calf muscle atrophy can reduce plantarflexion torque by up to 30%, forcing the knee and hip to compensate during running. Rebuilding the tendon requires a structured heavy slow resistance protocol to restore stiffness and strength.
Clinical metrics tracking Achilles tendon injury recurrence and rehabilitation:
- 1Recurrence RateApproximately 5% of professional athletes suffer a recurrent Achilles rupture, often due to inadequate tendon stiffness.
- 2Plantarflexion DeficitCalf muscle wasting following surgery can reduce ankle push-off force by up to 30% if not addressed.
- 3Tendon Stiffness ImprovementProgressive Heavy Slow Resistance training can increase tendon stiffness by 25% over a 12-week period.
- 4Rugby Return TimelineReturning to professional contact sports safely requires a minimum of 9 to 12 months of reconditioning.
The Clinical Opinion: Avoid Aggressive Passive Stretching
"Following a recurrent rupture, the temptation is to stretch the calf muscles to regain ankle mobility. My clinical opinion is that aggressive passive stretching in the first 3 months should be strictly avoided. Stretching a healing, scarred tendon can lengthen the tissue, permanently reducing its springiness and power. Instead, we must rely on controlled loading under weight to build length and strength simultaneously, ensuring the tendon remains tight and springy."
The 3-Step Tendon Stiffness Protocol
Rebuilding a twice-ruptured tendon requires moving from static muscle activation to heavy, slow resistance and progressive impact drills.
Phase 1: Early Isometric Loading and Range Protection
In the first 6 weeks post-surgery, protect the repair by avoiding any positions where the foot is pulled upward past neutral. Perform seated isometric calf presses against a solid block, holding the contraction for 10-15 seconds. This early loading stimulates collagen remodeling without stretching the healing tissue. Perform 5 repetitions, 3 times daily, focusing on a strong but pain-free contraction.
Phase 2: Heavy Slow Resistance (HSR) and Eccentric Heel Drops
Once the tissue has healed (weeks 8-16), begin progressive weight-bearing exercises to build muscle volume and tendon stiffness. Utilize a leg press or calf raise machine to perform slow heel raises: raise up over 3 seconds, hold for 2 seconds, and lower down over 4 seconds. Focus on this eccentric calf strengthening to help align the new collagen fibers. Perform 3 sets of 8 repetitions with a heavy, controlled weight, 3 times weekly.
Phase 3: Plyometric Power and Kinematic Drills
After week 20, begin retraining the tendon to absorb and release energy quickly. Start with light double-leg hopping, focusing on spending as little time on the ground as possible. Progress to single-leg bounds and lateral cuts, ensuring the ankle, knee, and hip remain aligned to avoid twisting. This high-speed training is essential for rebuilding tendon stiffness rehabilitation and preparing the body for the demands of rugby. Perform 2 sets of 10 seconds of hopping, twice weekly.
Restoring Lower Extremity Power
Rebuilding lower leg strength requires a comprehensive approach. Ensuring the glutes and quadriceps are strong helps distribute the forces of running and jumping, reducing the load on the Achilles tendon during explosive movements.
For more recovery guidelines, read our clinical breakdown of Achilles tendon loading protocols and view our article on restoring ankle stability after sprains. To learn how foot biomechanics impact the Achilles, see our guide on plantar fasciitis heel recovery to support your entire leg alignment.
Featured image attribution: Left panel photo of Xavier Coates adapted from Storm machine, licensed under CC BY-SA 4.0. Right panel displays a clinical 3D rendering of human ankle Achilles tendon rupture. Prepared for AyurPhysio clinical reference.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
