"The Achilles tendon acts like a heavy-duty steel spring launcher. When you pull the spring back during deceleration, it stores potential energy, but if the spring has a microscopic tear, the high-tension release will cause it to snap."
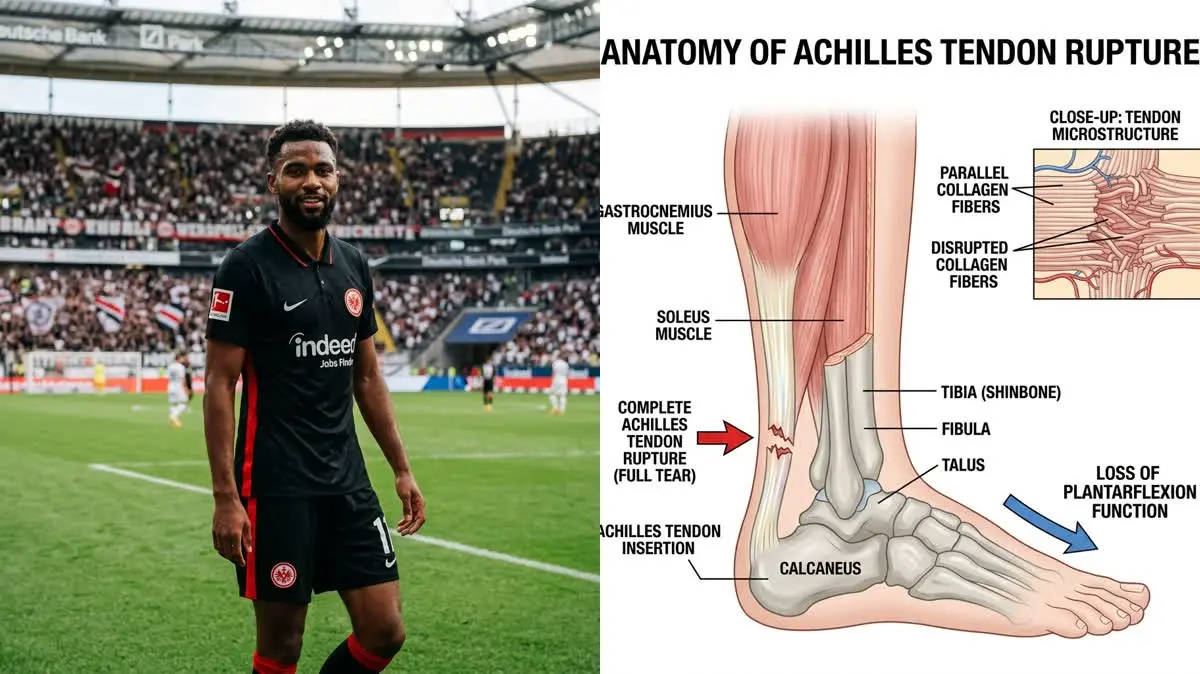
The sports world was shocked by the news that Eintracht Frankfurt's young French striker Hugo Ekitiké suffered a complete Achilles tendon rupture during pre-season training. This severe injury has sidelined the rising star for several months, disrupting his preparation for the upcoming international matches. For an explosive forward whose style relies on sudden acceleration, rapid cuts, and high-impact jumping, restoring tendon stiffness is a critical recovery goal.
Standard recovery for an Achilles rupture often involves long periods of immobilization in a plaster cast, which leads to calf muscle atrophy and ankle stiffness. However, for an elite footballer, a passive recovery approach delay return-to-sport timelines and increases re-injury risks. Modern sports physical therapy focuses on early weight-bearing and progressive mechanical loading to promote active tendon healing.
Restoring a ruptured tendon to handle explosive athletic loads requires a deep understanding of collagen modeling and lower extremity biomechanics. By applying precise forces through the kinetic chain and using targeted hugo ekitike injury rehabilitation, we can rebuild a stronger leg. This article analyzes the forces that cause tendon failure and details the clinical stages of calf reconditioning.
The Biomechanics of Explosive Acceleration and Achilles Load
The Achilles tendon is the thickest and strongest tendon in the human body, connecting the gastrocnemius and soleus muscles to the calcaneus bone. During running and jumping, this tendon acts as a powerful energy storehouse, absorbing energy when landing and releasing it during push-off. In elite soccer, the tendon experiences loads up to ten times the athlete's body weight during rapid cutting and deceleration.
A rupture typically occurs when the foot is dorsiflexed while the calf muscles contract forcefully, creating a sudden shearing stress. This motion usually happens during a quick sprint start, a high jump, or a sudden change of direction on the pitch. The force exceeds the tendon's ultimate tensile strength, leading to a complete tear of the thick collagen bundle.
Clinical studies show that Achilles tendon ruptures account for about 8% of all athletic injuries, with the highest occurrence in pivoting sports. Furthermore, up to 75% of these ruptures occur in soccer players during explosive deceleration movements on grass pitches. Rebuilding the tendon requires a careful balance between tissue protection and progressive mechanical loading.
Clinical metrics tracking Achilles tendon healing and calf muscle recovery:
- 1Peak Mechanical LoadThe Achilles tendon experiences forces up to 10 times body weight during high-speed deceleration.
- 2Calf Muscle AtrophyProlonged immobilization leads to a 25% loss in calf muscle volume within four weeks.
- 3Tendon Remodeling TimeThe biological process of tendon remodeling requires 9 to 12 months to restore full stiffness.
- 4Re-injury Risk ReductionControlled early weight-bearing reduces the risk of tendon re-rupture by 3.5 times.
The Clinical Opinion: Early Mobilization vs. Casting
"Following surgical repair of an Achilles tendon, the biggest challenge is preventing muscle atrophy and restoring dynamic dorsiflexion mobility. In my clinical opinion, placing the foot in a rigid cast for six weeks is outdated and leads to chronic calf weakness. We must start early weight-bearing in a functional brace with heel lifts within the first two weeks to stimulate tendon alignment."
Early functional mobilization applies mild tension to the healing tendon, which triggers the alignment of new collagen fibers along the line of stress. In contrast, total immobilization causes the new collagen to lay down in a disorganized pattern, making the tendon weak and prone to re-injury. By introducing early movement, we preserve the sliding mechanism of the tendon and prevent adhesions to the surrounding skin.
Furthermore, early weight-bearing helps maintain the strength of the calf muscles, specifically the soleus, which is the primary stabilizer during running. Protecting the soleus from wasting is critical because it handles the majority of the load during slow deceleration movements. A progressive loading program is the key to restoring this muscular support and protecting the joint.
Multi-Stage Achilles Rehabilitation Protocol
Rebuilding the Achilles tendon requires a progressive protocol that respects tendon tissue healing times while restoring ankle mobility.
Phase 1: Protection and Controlled Loading (Weeks 1-4)
In the first month post-surgery, the primary goals are to protect the surgical repair, reduce swelling, and begin partial weight-bearing. The patient wears a walking boot with three heel wedges to keep the foot in a slightly pointed position (plantarflexion). This position reduces the tension on the healing Achilles tendon and prevents excessive stretching of the repair site.
We begin gentle active foot movements, limiting movement to pointing the toes and moving the ankle inward. Passive stretching of the calf is strictly avoided during this phase to prevent stretching out the healing tendon. The patient performs isometric contractions of the calf muscles, gently pressing the foot down against a strap for 5 seconds.
Phase 2: Progressive Weight-Bearing and Strengthening (Weeks 6-12)
Once early healing is confirmed, we gradually remove the heel wedges from the walking boot, one wedge every two weeks. We transition the patient to normal shoes and begin double-leg calf raises on a flat surface, focusing on the lift. We gradually introduce eccentric heel drops, where the patient stands on a step and lowers their heels slowly over 4 seconds.
This eccentric loading is crucial because it applies controlled tension that stimulates the remodeling of collagen fibers. The patient performs 3 sets of 10 repetitions, three times per week, staying within a pain-free range. We also incorporate balance exercises, such as single-leg standing on a foam pad, to rebuild ankle stability and joint position sense.
Phase 3: Plyometric Drills and Sports-Specific Training (Weeks 16-24)
This final phase focuses on rebuilding explosive strength and soccer-specific deceleration mechanics. We begin double-leg hopping drills on a soft surface to absorb landing forces. We progress to single-leg hops and lateral cutting movements that mimic competitive play.
We introduce linear running, gradually increasing speed and adding sudden stop-and-go drills to test the tendon's stiffness. We monitor the calf circumference and tendon thickness to ensure the tissues are adapting well to the increased loads. The athlete performs these plyometric sessions twice weekly, allowing 72 hours of recovery between workouts.
Kinetic Chain Integration
An Achilles tendon rupture affects the mechanics of the entire lower body, leading to hip compensations. Weakness in the calf muscles forces the hip muscles and lower back to work harder. The rehabilitation program must include gluteus medius and hamstring conditioning.
For more recovery guidelines, read our detailed guide on Achilles tendinitis heavy slow resistance protocols and view our breakdown of spinal extension rehab. To understand knee stability, check our analysis of meniscus shear stress rehabilitation and ACL reconstruction milestone protocols. To learn about calf muscle mechanics, view our analysis of soleus calf strain recovery in basketball players.
Featured image attribution: Left panel photo of Hugo Ekitiké adapted from Wikimedia Commons page (File:Hugo Ekitike 2023.jpg). Right panel displays a clinical anatomical diagram of Achilles tendon rupture. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
