"Explosive acceleration in a large frame requires a perfect balance of pelvic stiffness and muscular elasticity. When the core fails to anchor the pelvis, the hip flexors are forced to operate at extreme lengths, turning a routine stride into a structural tear."
Erling Haaland's massive frame and explosive acceleration make him one of the most dominant strikers in world football. However, generating that level of force puts immense strain on his musculoskeletal system. When a player of his size suffers a hip flexor strain, it highlights the delicate biomechanical balance required for high-velocity acceleration.
Standard athletic recovery often relies on rest and passive therapy. However, for a high-performance athlete, prolonged inactivity causes muscle imbalances and joint stiffness. Reconditioning the hip requires a structured approach that addresses the exact mechanical forces acting on the pelvic ring.
Restoring elite sprinting performance requires dissecting the mechanics of the injury. By studying muscle recruitment patterns and using targeted erling haaland injury rehabilitation, we can rebuild a highly stable pelvis.
This article reviews the biomechanics of hip flexor trauma, clinical rehabilitation stages, and pelvic stabilization protocols.
The Biomechanics of Sprinter Acceleration and Hip Flexor Trauma
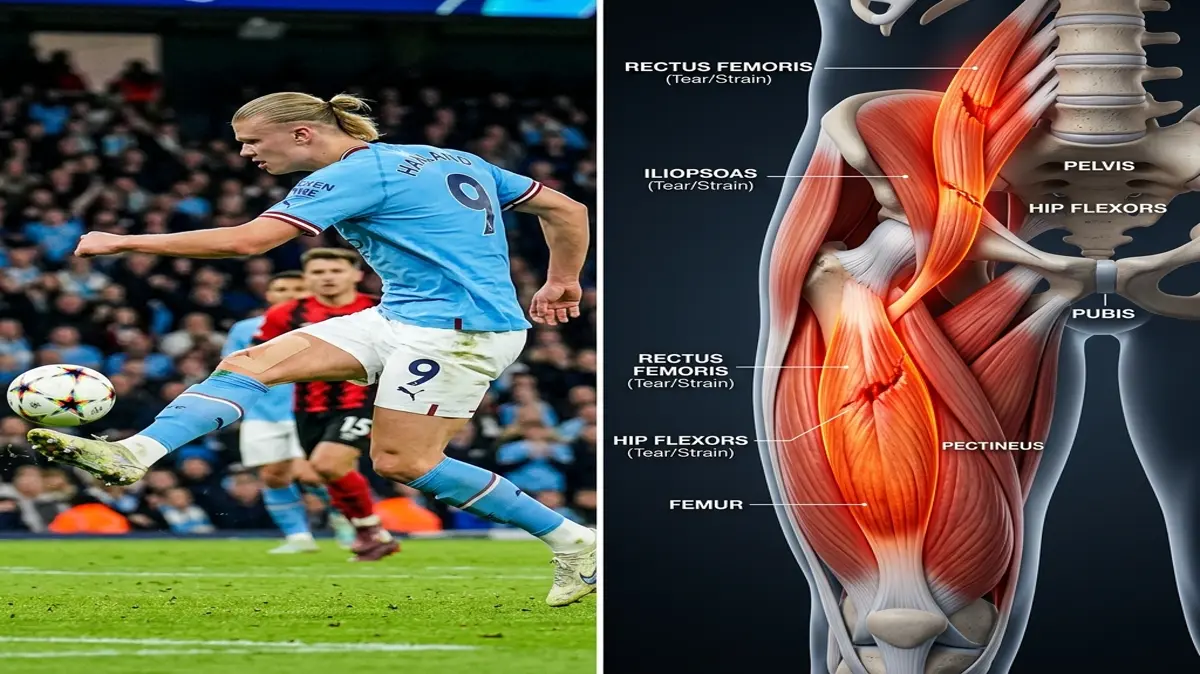
During the acceleration phase of a sprint, the hip flexor complex undergoes a rapid transition from high-load eccentric lengthening to powerful concentric shortening. As the leg reaches back in the terminal extension phase, the rectus femoris and iliopsoas are stretched under load to decelerate the leg. This eccentric loading places extreme tension on the muscle fibers.
Immediately after decelerating, the hip flexors contract concentrically to pull the thigh forward into the swing phase. This rapid contraction cycle generates forces that can exceed the muscle's structural threshold. If the pelvic stabilizers fail to maintain a neutral position, the hip flexors are placed in a mechanically vulnerable state, leading to microscopic tissue tears at the myotendinous junction.
Without proper rehabilitation, these micro-tears heal with rigid, disorganized scar tissue. This inelastic tissue reduces the muscle's capacity to absorb force, predisposing the athlete to recurrent strains. Compensatory movement patterns quickly develop, stressing the contralateral hip and lower back.
Hip strains represent up to 10% of all professional soccer injuries. Furthermore, recurrent strains account for nearly 15% of these cases, leading to extended recovery times. Restoring performance requires progressive eccentric loading to align the healing muscle fibers along their normal line of pull.
Key clinical parameters for assessing hip flexor recovery and pelvic stability:
- 1Injury PrevalenceHip and groin strains make up approximately 10% of all muscle injuries in professional soccer.
- 2Strength DeficitA hip flexor strength deficit of over 10% compared to the uninjured side increases re-injury risk by 50%.
- 3Tissue Remodeling WindowControlled eccentric loading must be introduced by week 3 to promote aligned scar tissue formation.
- 4Pelvic AlignmentReducing anterior pelvic tilt by 5 degrees significantly unloads the anterior hip structures during terminal extension.
The Clinical Opinion: Active Progressive Loading vs. Passive Rest
"Treating a hip flexor strain in an explosive athlete requires early, controlled loading rather than prolonged rest. In my clinical opinion, passive recovery leads to disorganized collagen repair and muscle atrophy. By introducing sub-maximal isometric holds within the first week, we stimulate cellular repair and preserve pelvic control, laying the foundation for high-velocity sprinting."
Traditional recovery protocols often overemphasize absolute rest. While rest decreases acute pain, it allows the injured muscle to heal in a shortened, weak state. In contrast, modern physical therapy introduces mechanical tension early to guide the alignment of new tissue fibers.
Early isometric contractions stimulate local blood flow and cellular protein synthesis without placing excessive shear stress on the healing tear. As the tissue strengthens, we progress to eccentric exercises, which train the muscle to absorb force while lengthening. This training is essential for preventing future re-injury during sprinting.
Multi-Stage Hip Flexor and Pelvic Rehabilitation Protocol
Reconditioning a soccer player's hip requires a structured progression that builds tissue tolerance while restoring pelvic core integration.
Phase 1: Protection and Isometric Activation (Weeks 1-2)
The initial phase focuses on reducing inflammation, protecting the healing fibers, and introducing gentle activation. The athlete avoids activities that require explosive hip flexion or extreme extension stretching. Ice and compression are applied daily to manage swelling.
Sub-maximal isometric holds are performed in a neutral hip position to maintain muscle activation. The athlete lies on their back and presses their knee against manual resistance for 5 seconds. This exercise is performed in 3 sets of 10 repetitions twice daily.
Pelvic neutral drills are introduced to engage the core. The athlete performs posterior pelvic tilts in a lying position to activate the deep abdominal muscles. Maintaining a neutral pelvis reduces the baseline tension on the rectus femoris.
Phase 2: Concentric Loading and Core Integration (Weeks 3-4)
Once the athlete can perform isometric holds without pain, we progress to active concentric movements. The athlete performs standing hip flexion exercises using a light resistance band. These exercises are performed through a comfortable, controlled range of motion.
Core stabilization exercises are progressed to bridge variations. The athlete performs single-leg glute bridges to strengthen the posterior chain while maintaining pelvic alignment. This exercise helps balance the front-to-back forces acting on the pelvis.
Gentle eccentric loading begins with slow, controlled leg lowering. The athlete raises their leg concentrically, then lowers it over a 5-second count. This eccentric activation prepares the muscle for the high-deceleration forces of sprinting.
Phase 3: Eccentric Power and Sports-Specific Speed (Weeks 5-8)
The final phase focus is on restoring high-velocity eccentric strength and soccer-specific movement patterns. The athlete performs eccentric hip flexor exercises, such as the slider lunge, focusing on a slow, controlled descent. These exercises are performed with progressive resistance.
Running drills begin on a linear path, starting at 50% velocity and gradually increasing as tolerated. We monitor the hip closely for any tightness during deceleration. The athlete performs acceleration-deceleration drills twice weekly.
High-velocity soccer drills, including rapid directional changes and kicking, are introduced. These dynamic movements ensure the hip flexor complex can handle the extreme rotational forces of competitive play.
Preventing Kinetic Chain Imbalances
A hip flexor injury does not occur in isolation; it is deeply connected to pelvic and spinal mechanics. Tightness in the hip flexors restricts hip extension, forcing the lumbar spine to hyperextend to compensate. This compensation strains the lower back joints, leading to secondary pain.
To prevent these kinetic chain issues, the rehabilitation program incorporates deep core and gluteus medius activation. Maintaining strength in these supporting muscle groups ensures optimal pelvic control. A balanced kinetic chain is the key to achieving long-term athletic durability.
For more lower extremity recovery guidelines, read our detailed guides on groin strain and adductor rehab, FAI safe squat mechanics, and post-operative ACL rehabilitation timelines. To understand athletic calf and hamstring biomechanics, view our analyses of Giannis Antetokounmpo's soleus strain and Elly De La Cruz's hamstring sprint deceleration mechanics. You can also review Zlatan Ibrahimovic's knee compensation analysis.
Featured image attribution: Left panel displays a visual representation of football player Erling Haaland in action. Right panel shows a clinical 3D medical illustration highlighting the hip flexor muscle group (rectus femoris, iliopsoas) and surrounding pelvic structure. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
