"Returning to elite contact sports after sudden cardiac arrest is one of the most complex challenges in sports medicine. It requires a flawless convergence of cardiac electrophysiology, device mechanics, and highly precise cardiorespiratory reconditioning to ensure safety at maximal workload."
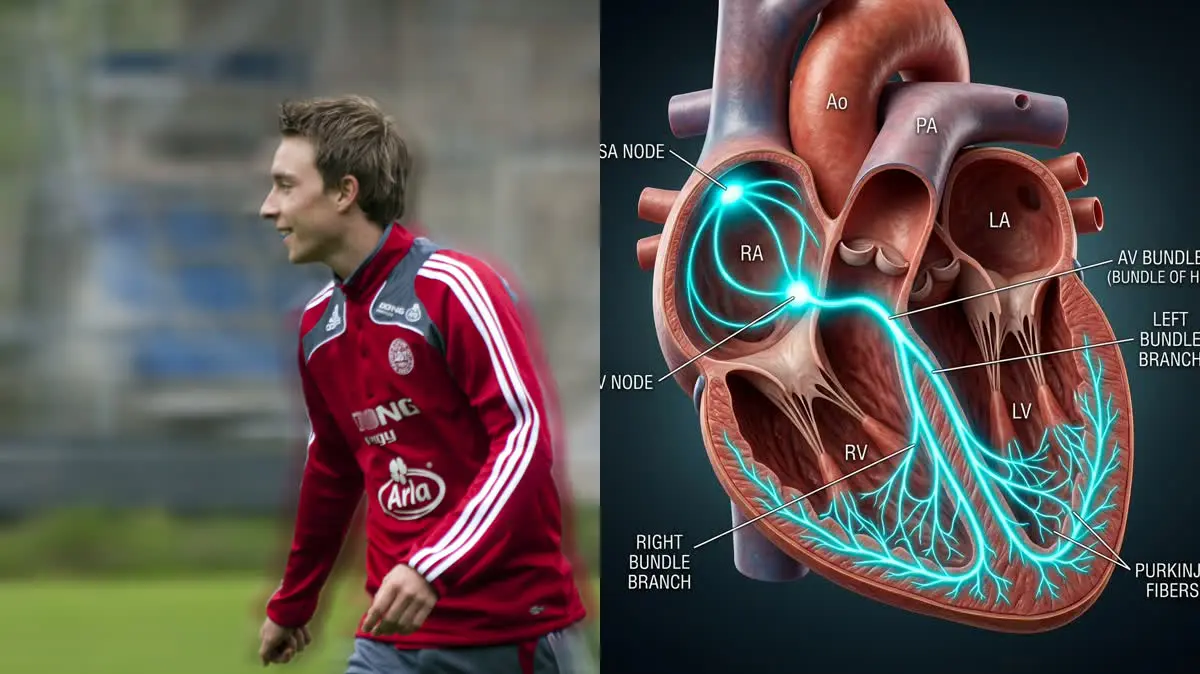
In one of the most dramatic and emotionally charged moments in modern sports history, Danish football star Christian Eriksen suffered a sudden cardiac arrest on the pitch during Euro 2020. The midfielder collapsed unexpectedly, requiring immediate cardiopulmonary resuscitation (CPR) and emergency defibrillation to save his life. Following his stabilization, Eriksen was fitted with an Implantable Cardioverter-Defibrillator (ICD). His subsequent return to elite competitive football in the English Premier League and international tournaments challenged decades of conservative medical consensus and redefined the limits of sports cardiology.
Eriksen's journey has sparked intense scientific interest in how the athletic heart adapts to extreme physical training, the mechanics of ICD devices under high-impact conditions, and the rehabilitation protocols necessary for patients recovering from major cardiac events. In this clinical evaluation, we will analyze the physiology of sudden cardiac arrest in athletes, investigate the structural adaptations of "athletic heart syndrome," detail the biomechanical implications of playing sports with an ICD, and outline a multi-phase cardiorespiratory reconditioning protocol designed to return high-performance athletes to safe play.
The Pathophysiology of Sudden Cardiac Arrest vs. Heart Attack
To understand the mechanics of Eriksen's recovery, it is crucial to distinguish between two frequently confused cardiovascular events: a myocardial infarction (heart attack) and Sudden Cardiac Arrest (SCA). A heart attack is a plumbing problem, where blood flow to a portion of the heart muscle is blocked, typically due to coronary artery disease, leading to localized tissue ischemia. In contrast, sudden cardiac arrest is an electrical problem. It occurs when the heart's electrical system malfunctions, causing the ventricles to beat rapidly and chaotically—a state known as ventricular fibrillation (VF) or ventricular tachycardia (VT).
During ventricular fibrillation, the heart muscle quivers ineffectively instead of pumping blood to the brain and vital organs. Without immediate intervention, death occurs within minutes. In young, highly trained athletes, sudden cardiac arrest is rarely caused by standard coronary artery blockages. Instead, it is typically triggered by silent, underlying structural or electrical abnormalities, including:
- Hypertrophic Cardiomyopathy (HCM): An abnormal thickening of the left ventricular wall, which can disrupt the heart's electrical pathways and cause fatal arrhythmias during intense exercise.
- Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC): A genetic condition where healthy heart muscle in the right ventricle is replaced by fat and fibrous tissue, creating electrical instability.
- Myocarditis: Inflammation of the heart muscle, often triggered by a common viral infection, which can create temporary electrical focal points prone to triggering arrhythmias.
- Congenital Coronary Artery Anomalies: Structural deviations in the origin or course of the coronary arteries that can restrict blood flow under high-stress conditions.
- Sudden cardiac arrest is the leading cause of non-traumatic death in young athletes, occurring in approximately 1 in 50,000 to 1 in 80,000 athletes annually.
- For every minute that defibrillation is delayed during ventricular fibrillation, the likelihood of survival decreases by 7% to 10%.
- The international ICD Sports Registry tracked over 400 competitive athletes with ICDs for several years, reporting zero deaths or resuscitations during sports participation.
- Cardiorespiratory fitness, as measured by VO2 max, can decline by 20% to 30% within just four to six weeks of absolute physical inactivity.
Athletic Heart Syndrome: Physiological Adaptation or Pathology?
The human heart is highly adaptable. In response to regular, high-intensity aerobic and anaerobic training, it undergoes structural changes collectively termed Athletic Heart Syndrome. These adaptations are physiological responses designed to increase cardiac output and meet the oxygen demands of active skeletal muscles. Key characteristics include:
Eccentric Left Ventricular Hypertrophy: An increase in both the chamber size (cavity diameter) and wall thickness of the left ventricle, allowing the heart to hold and pump more blood per beat (increased stroke volume).
Sinus Bradycardia: A slow resting heart rate (often below 40 beats per minute) caused by high vagal tone. Because the heart pumps more blood per contraction, it can beat fewer times per minute to maintain resting cardiac output.
This physiological hypertrophy can sometimes overlap with hypertrophic cardiomyopathy, creating a diagnostic challenge known as the "grey zone." Clinicians use advanced imaging (such as cardiac MRI) and detraining protocols to monitor whether the heart tissue returns to normal, distinguishing benign athletic changes from dangerous pathological disease.
"For an athlete fitted with an ICD, returning to sport requires a collaborative medical clearance process. We must program the device with a customized heart rate detection zone. The maximum heart rate achieved during competitive play must remain at least 15 to 20 beats per minute below the ICD's shock threshold. This safety margin prevents the delivery of an inappropriate shock during high-intensity exercise when the heart rate naturally climbs to near-maximal levels. Additionally, physical contact at the implant site must be prevented using custom carbon-fiber chest shields."
The Role and Biomechanics of the ICD in Return to Play
An Implantable Cardioverter-Defibrillator (ICD) is a small, battery-powered device surgically placed under the skin, typically below the collarbone. It monitors the heart's rhythm through thin wires (leads) threaded into the cardiac chambers. If the device detects a lethal arrhythmia like ventricular fibrillation, it delivers an electrical shock to restore a normal rhythm.
Historically, guidelines like the Bethesda Conference consensus prohibited athletes with ICDs from participating in competitive, high-velocity sports. The primary concern was that the extreme movements of sports could damage the device leads, dislodge the generator, or cause the device to deliver unnecessary shocks due to rapid heart rates. However, modern registries have shown that with proper device configuration, appropriate padding, and structured physical rehabilitation, return to play is feasible and safe for selected athletes.
From a biomechanical perspective, the rehabilitation process must address the physical presence of the device. The surgical incision and tissue pocket can restrict shoulder mobility and alter upper body biomechanics. Early movement must balance the need to preserve shoulder range of motion with the critical requirement to allow the lead wires to scar and anchor securely into the heart wall, avoiding displacement.
The Cardiorespiratory and Sports Biomechanics Rehab Protocol
Reconditioning an athlete after cardiac arrest requires a structured approach that prioritizes cardiovascular safety while rebuilding athletic capacity.
- 1Phase 1: Controlled Mobility and Low-Intensity Base (Weeks 1–4)Focus on restoring gentle shoulder range of motion on the implant side, limiting arm elevation to 90 degrees to protect lead integrity. Begin low-intensity cardiovascular conditioning, such as walking or stationary cycling, keeping the heart rate strictly below 60% of the patient's age-predicted maximum. All exercises must be performed under continuous heart rate monitoring.
- 2Phase 2: Moderate Aerobic Base and Core Stabilization (Weeks 5–8)Progress cardiovascular exercise to 60-70% of maximum heart rate, introducing longer durations. Incorporate core stabilization exercises and closed-chain lower body movements like leg presses and squats. Reintroduce full shoulder mobility exercises, focusing on restoring symmetrical movement without placing excessive strain on the ICD site.
- 3Phase 3: High-Intensity Intervals and Agility Drills (Weeks 9–12)Introduce short intervals of high-intensity aerobic exercise, monitoring cardiac response closely. Add sport-specific agility drills, including lateral cuts, acceleration, and deceleration. Introduce dynamic upper body movements, and begin testing custom chest protectors to ensure comfort and stability during athletic maneuvers.
- 4Phase 4: Sport Integration and Competitive Clearance (Weeks 13+)Gradually integrate the athlete into contact drills and team training sessions, using protective gear over the ICD. Perform a maximal cardiopulmonary exercise test (CPET) to confirm that no arrhythmias occur at peak workload. Establish a clear emergency response plan, including the presence of an automated external defibrillator (AED) at all sessions.
Synergy in Sports Recovery and Heart Health
Rebuilding after a major health event requires a holistic view of the body's systems, balancing cardiorespiratory performance with musculoskeletal health. To explore how traditional systems analyze cardiac vitality and stress management, read our clinical review of Jeremy Clarkson's heart health and coronary artery disease. For an investigation into managing acute systemic crises and recovery protocols, study our evaluation of Bonnie Tyler's appendix rupture and post-cardiac arrest recovery. Additionally, if you are managing complex physical traumas alongside cardiorespiratory care, consult our comprehensive guide on Jeremy Renner's trauma rehabilitation pathways.
Christian Eriksen's return to elite football is a testament to the resilience of the human body and the precision of modern medicine. By following a structured cardiorespiratory reconditioning program, monitoring heart rates carefully, and ensuring the mechanical integrity of protective devices, athletes can overcome significant cardiac events. The key to success lies in matching medical management with physical rehabilitation, protecting the heart while rebuilding the athletic foundation for long-term health.
Featured image: Clinical side-by-side composite showing Christian Eriksen (left) and an anatomical 3D rendering of the human heart showing an ICD lead placement (right). Created for AyurPhysio editorial use. Wikimedia Commons attribution: Christian Eriksen image by Paul Blank licensed under CC BY-SA 3.0. Modified by cropping and compositing.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
