"The thoracic spine is like the mast of a sailboat. If the mast is locked in place and cannot bend or rotate, the strong winds will transfer all the stress down to the rigging, causing the ropes to snap."
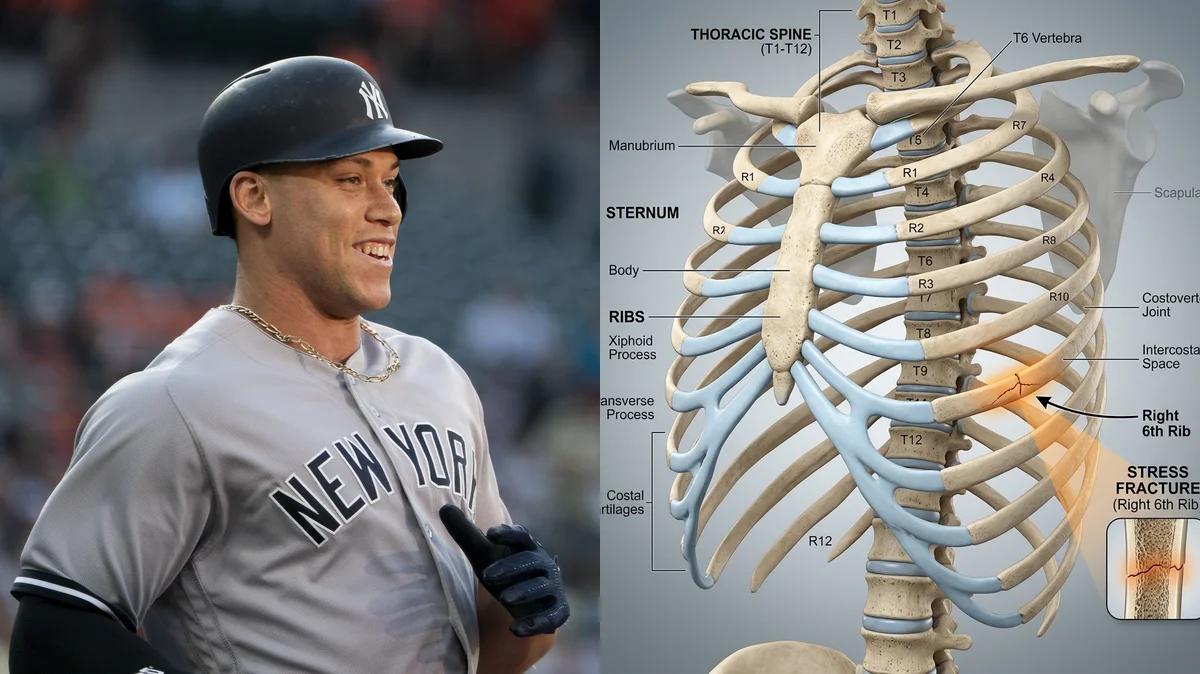
When New York Yankees superstar Aaron Judge was sidelined with a persistent rib injury, diagnostic imaging revealed a stress fracture of the first right rib. For a power hitter whose swing generates immense rotational forces, this injury highlights the hidden physical costs of elite performance. Unlike acute fractures caused by collisions, a stress fracture develops slowly, resulting from repetitive muscular pull on the bone surface.
Standard treatment approaches that rely solely on rest often fail to address why the injury occurred in the first place. When an athlete returns to play without correcting imbalances in spinal rotation and core control, the same bone areas are subjected to excessive stress, leading to recurrence. To prevent chronic issues, rehabilitation must focus on restoring movement quality throughout the trunk.
To safely rebuild bone strength and return to swing velocity, we must target spinal mobility and muscular coordination. Through a detailed analysis of the aaron judge rib stress fracture, we can develop a matching recovery plan. This guide examines the mechanics of rotational stress and outlines the clinical steps to restore function.
The Biomechanics of Rotational Torque and Serratus Pull
A baseball swing is a complex movement that requires transferring energy from the ground up through the pelvis, torso, and arms. This transfer of force requires a high amount of rotational torque batting biomechanics. As the hitter rotates their trunk at high speeds, muscles like the serratus anterior and internal obliques contract powerfully to pull the rib cage forward.
The serratus anterior muscle originates on the upper ribs and inserts into the scapula. During a swing, this muscle pulls hard on the ribs to stabilize the shoulder blade and drive the arms forward. If the thoracic spine is stiff, the torso cannot rotate smoothly, forcing the ribs to absorb the excess twist. This repetitive serratus anterior muscle strain pulls on the bone structure, leading to micro-fractures over time.
Clinical statistics show that rib stress fractures account for up to 10% of all injuries in rotational sports like rowing and baseball. Over 85% of these injuries occur on the lead side of the torso, reflecting the asymmetrical loads of the swing. Correcting this imbalance requires active rib stress fracture rehabilitation and restoring thoracic mobility.
Clinical metrics tracking rib stress injury prevalence and recovery timelines:
- 1Lead-Side PrevalenceOver 85% of rotational rib stress fractures occur on the lead side of the trunk due to asymmetrical swing forces.
- 2Injury ProportionRib stress fractures account for up to 10% of all athletic injuries in sports requiring high-velocity torso rotation.
- 3Spinal Load ReductionRestoring thoracic spine rotation can reduce the shear force on the rib cage by 30%.
- 4Bone Healing WindowThe average recovery timeline for a non-displaced rib stress fracture is 6 to 8 weeks of rest.
The Clinical Opinion: Restore Thoracic Spine Rotation
"A rib stress fracture is rarely just a bone problem; it is almost always a spinal mobility problem. When the thoracic spine loses its ability to rotate, the ribs must bear the force of the swing. My clinical opinion is that we must focus on active thoracic spine mobility exercises and hip rotational control during recovery. Restoring movement in the middle back reduces the load on the ribs, protecting them from future fractures."
The 3-Step Rib Stress Recovery Protocol
Reconditioning the trunk requires protecting the healing bone, restoring joint mobility, and rebuilding rotational strength.
Phase 1: Bone Protection and Core Stabilization
During the first 4 weeks, avoid all rotational exercises, heavy lifting, and activities that cause pain. Focus on breathing exercises to maintain rib expansion and perform static abdominal holds (planks, deadbugs) to support the spine. This early core stabilization sports injury protocol keeps the trunk stable, minimizing movement at the fracture site to support early bone healing.
Phase 2: Thoracic Mobilization and Serratus Release
Once cleared for movement (weeks 6-8), begin gentle stretching to restore mobility to the middle back and chest. Perform foam roller extensions and side-lying thoracic open-book stretches, rotating the chest while keeping the hips still. Use light stretching to release tension in the serratus anterior and pectoral muscles. Perform these stretches twice daily, moving slowly and staying within a pain-free range.
Phase 3: Progressive Rotational Strength
After week 8, begin rebuilding the power needed for swinging. Start with light cable rotations, focusing on rotating through the upper back while keeping the lower back stable. Progress to medicine ball throws and light batting practice, gradually increasing swing speed. Focus on maintaining control throughout the movement, avoiding any sudden twisting. Perform 3 sets of 10 repetitions, 3 times weekly.
Preventing Recurrent Rotational Injuries
Restoring balance to the body is the key to long-term performance. Ensuring both hips have equal mobility and strengthening the oblique muscles helps distribute the forces of the swing evenly, protecting the ribs from overload.
For more recovery guidelines, read our article on thoracic and cervical spine reconditioning and view our guide on preventing spinal injuries through core stability. To learn about thoracic mobility exercises, read our breakdown of mid-back mobilization protocols to support your entire athletic framework.
Featured image attribution: Left panel photo of Aaron Judge adapted from Keith Allison, licensed under CC BY-SA 2.0. Right panel displays a clinical 3D rendering of human thoracic cage stress fracture. Prepared for AyurPhysio clinical reference.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
