"The ACL is like the central seatbelt of the knee joint. When you slam on the brakes while turning, the seatbelt locks to keep the passenger from sliding forward off the seat. If that seatbelt snaps, the entire dashboard collapses."
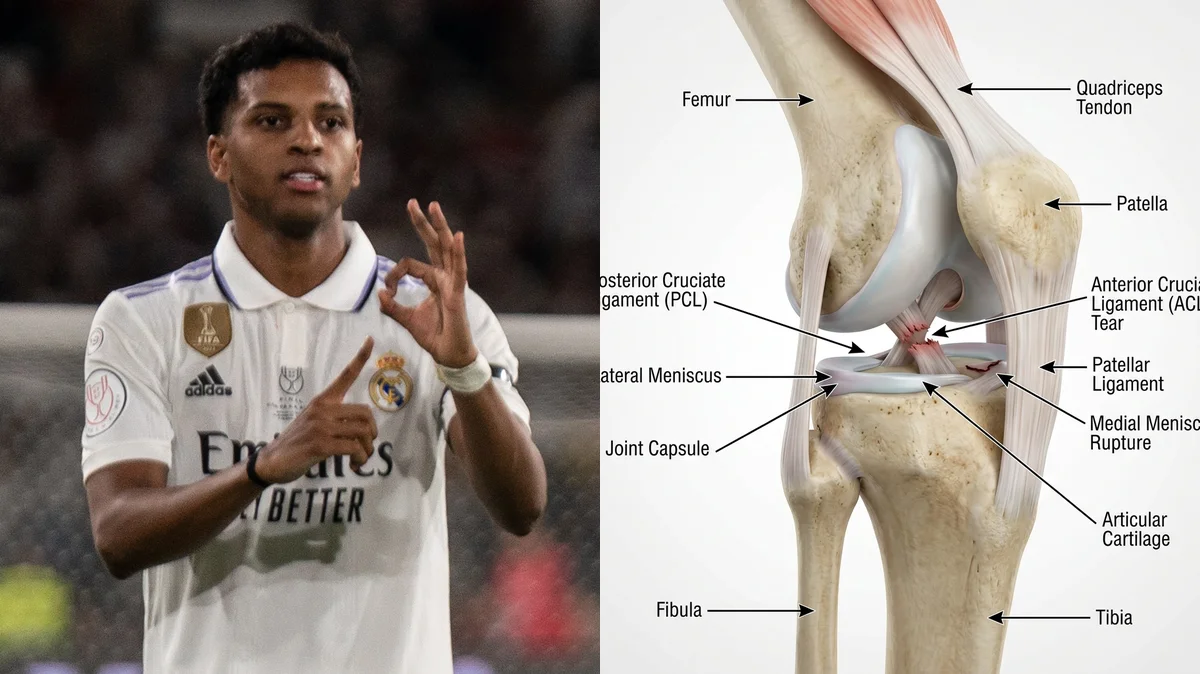
The news that Real Madrid and Brazilian winger Rodrygo Goes suffered a ruptured anterior cruciate ligament (ACL) and meniscus tear has sent shockwaves through the football community, sidelining him for the upcoming World Cup. This double-tissue failure represents one of the most demanding orthopedic challenges in modern sports medicine. For an elite player reliant on rapid deceleration, cutting, and explosive acceleration, rebuilding knee stability requires more than just standard surgical repair.
Standard rehabilitation programs often focus too heavily on basic straight-line movements early on, failing to prepare the knee for the multi-directional forces of competitive sports. When the primary ligament stabilizes and the shock-absorbing cartilage is damaged, the joint loses its mechanical defenses. Without structured progression, the athlete risks graft failure or chronic joint decay.
To ensure a complete and lasting return to performance, rehabilitation must address the underlying biomechanics of the injury. By understanding the forces that cause ligament failure and applying targeted rodrygo acl tear recovery protocols, we can restore joint integrity. This guide analyzes the mechanics of Rodrygo's injury and details the clinical stages of knee reconditioning.
The Biomechanical Breakdown of Valgus Collapse
An anterior cruciate ligament rupture typically occurs during high-speed deceleration combined with a sudden change of direction. When a player plants their foot and attempts to cut, the knee joint can experience a pattern known as knee valgus collapse. In this position, the knee caves inward, the tibia rotates externally, and the femur rotates internally under heavy gravitational loads.
This dynamic alignment creates a shearing force that stretches the ACL beyond its elastic limit. The ACL is designed to prevent the tibia from sliding too far forward relative to the femur, and to resist excessive rotation. When valgus collapse occurs, the ligament is forced to bear the full load of the body's momentum, leading to a complete tear. Concomitant meniscus shear stress rehabilitation is required because the lateral and medial meniscus are pinched between the shifting bone surfaces during the rupture.
Clinical statistics show that over 70% of ACL tears occur through non-contact mechanisms, highlighting the role of movement quality and muscle fatigue. Furthermore, concomitant meniscus tears are present in up to 60% of acute ACL ruptures, complicating early weight-bearing and range of motion guidelines. Restoring both structures requires a careful balance between tissue protection and progressive loading.
Clinical metrics tracking knee injury risk factors and rehabilitation outcomes:
- 1Non-Contact PrevalenceOver 70% of ACL ruptures occur during non-contact cutting, pivoting, or landing movements.
- 2Concomitant Meniscus DamageConcomitant meniscus tears occur in up to 60% of acute ACL tears due to high shear forces.
- 3Re-injury Risk FactorFailing to achieve symmetrical quadriceps strength before returning to sport increases re-injury risk by 4.5 times.
- 4Ligament Remodeling WindowThe full biological remodeling of an ACL graft (ligamentization) takes between 9 to 12 months.
The Clinical Opinion: Focus on Early Quadriceps Activation
"Following an anterior cruciate ligament reconstruction, the biggest obstacle to recovery is arthrogenic muscle inhibition, where the brain shuts down the quadriceps to protect the swollen joint. My clinical opinion is that we must target early quad activation using neuromuscular electrical stimulation and isometric holds within the first post-operative week. Allowing the quads to atrophy early on lengthens the recovery timeline and alters patellofemoral tracking, creating chronic pain."
Multi-Stage Knee Reconditioning Protocol
Reconditioning the knee requires a step-by-step approach that respects tissue healing timelines while rebuilding the kinetic chain.
Phase 1: Restoring Extension and Quad Activation
In the first 4 weeks post-surgery, the primary goals are to eliminate joint swelling, regain full passive knee extension, and re-establish quadriceps control. Perform straight leg raises with a focus on locking the knee straight at the top. Use neuromuscular electrical stimulation to assist the quadriceps contraction if needed. To protect the meniscus repair, limit knee flexion to 90 degrees during this early stage, and maintain partial weight-bearing with crutches as directed.
Phase 2: Progressive Loading and Closed-Kinetic Chain strength
Once the graft is stable and the meniscus has healed (weeks 6-12), progress to weight-bearing exercises to build muscle volume. Perform goblet squats, leg presses, and step-ups, keeping the knee aligned over the second toe to avoid valgus collapse. Emphasize eccentric control, lowering the weight slowly over 3-4 seconds. Begin bilateral heel raises to rebuild calf strength and support the posterior knee joint. Perform 3 sets of 8-12 repetitions, 3 times weekly.
Phase 3: Rotational Control and Plyometric Drills
After week 16, start rebuilding rotational stability and explosive strength. Begin with double-leg landing drills off a low box, focusing on absorbing impact softly. Progress to single-leg hops and lateral shuffling to retrain the lateral stabilizers (gluteus medius and peroneals). This lateral control is essential for preventing valgus collapse during sudden changes of direction. Perform 3 sets of 5 repetitions per leg, twice weekly, ensuring perfect knee alignment on every landing.
Restoring the Kinetic Chain
Successful rehabilitation requires looking beyond the knee joint itself. Hip weakness and ankle stiffness often contribute to valgus collapse, so restoring hip abduction strength and ankle dorsiflexion mobility is crucial for long-term joint health.
For more recovery guidelines, read our detailed guide on ACL post-surgery milestone protocols and view our breakdown of meniscus rehabilitation strategies. To understand the role of hip stability, read our analysis of gluteus medius conditioning to support your entire lower extremity alignment.
Featured image attribution: Left panel photo of Rodrygo adapted from Suraal, licensed under CC BY-SA 2.0. Right panel displays a clinical 3D knee model showing ACL tear and meniscus rupture. Prepared for AyurPhysio clinical reference.
Dr. Dhanushika Dilshani
Expert Ayurvedic Wellness Doctor. Specialized in modern holistic wellness, optimizing dermal resilience, cosmetic radiance, and systematic diagnosis driven by traditional and evidence-based medical logic.
Medical Disclaimer
The information provided by AyurPhysio is for general educational and informational purposes only. It is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health providers with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Trending Guides
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity
4 min readHarry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
4 min readKarim Benzema's Daily Routine: Cupping Therapy (Hijama) and HIIT Conditioning
4 min readNeymar Jr.'s Daily Routine: Joint Stabilization and Hyperbaric Oxygen Therapy
4 min readMohamed Salah's Daily Routine: Early Morning Conditioning and Hyperbaric Recovery
4 min readWeekly Wellness
Don't miss the next guide
Get holistic health tips and new guides delivered to your inbox.
Related Healing Guides
View All Guides →
Luka Modrić's Daily Routine: Low-Impact Resistance Training and Midfield Longevity

Harry Kane's Daily Routine: Hamstring Preservation and Anti-Inflammatory Nutrition
